BEFORE WE left Baltimore, we had been told that, because of my Karen missionary ancestors, we would be stationed in Loikaw, in the Karenni States, where the people understood the Sgaw Karen which I spoke before I learned English. We had accordingly studied up all the known facts about the Red Karens, the Padaungs who stretch the necks of their women with brass rings till they are about a foot long, about that special variety of Karens that does not permit its men to marry outside of their own village and is thereby rapidly dying out, and about the other funny people of the Karenni. When we reached New York we were told that the mission could no longer afford---the missionary revival that had followed the first World War had already lost momentum---to put a medical missionary at Loikaw, and we would have to go to Kengtung, the largest and easternmost Shan State that borders on China, Indo-China and Siam.
I didn't care. All I wanted was plenty of jungle and thousands of sick people to treat, preferably with surgery. Our luck broke when we changed steamers at Liverpool and found, as a fellow passenger, Mr. John Shaw, who had been the Burma government's assistant superintendent of Kengtung State. Mr. Shaw had a very attractive personality and spent a great deal of time on the long voyage telling us all he knew about Kengtung. Full of Kengtung dreams we finally disembarked in Rangoon, where Leslie and Tiny both promptly came down with dengue fever after the minimum incubation period of three days.
Dr. Harper was in Rangoon when we arrived. The mission committee had a session and Dr. Harper, for Namkham, and Dr. Henderson, for Kengtung, went into a tussle to see who could get us. Dr. Harper won by promising me his practice, all his good will, and a free hand, since he was going to retire permanently in the spring. The committee agreed and ordered me to Namkham. That seemed a most appropriate decision in view of my infantile fascination for Dr. Harper and all his works. The committee was anxious that Tiny remain in Rangoon till our son was born, two months later. But Tiny, in spite of dengue fever was so anxious to get to the place where we would at last have our own home that she voted to start at once.
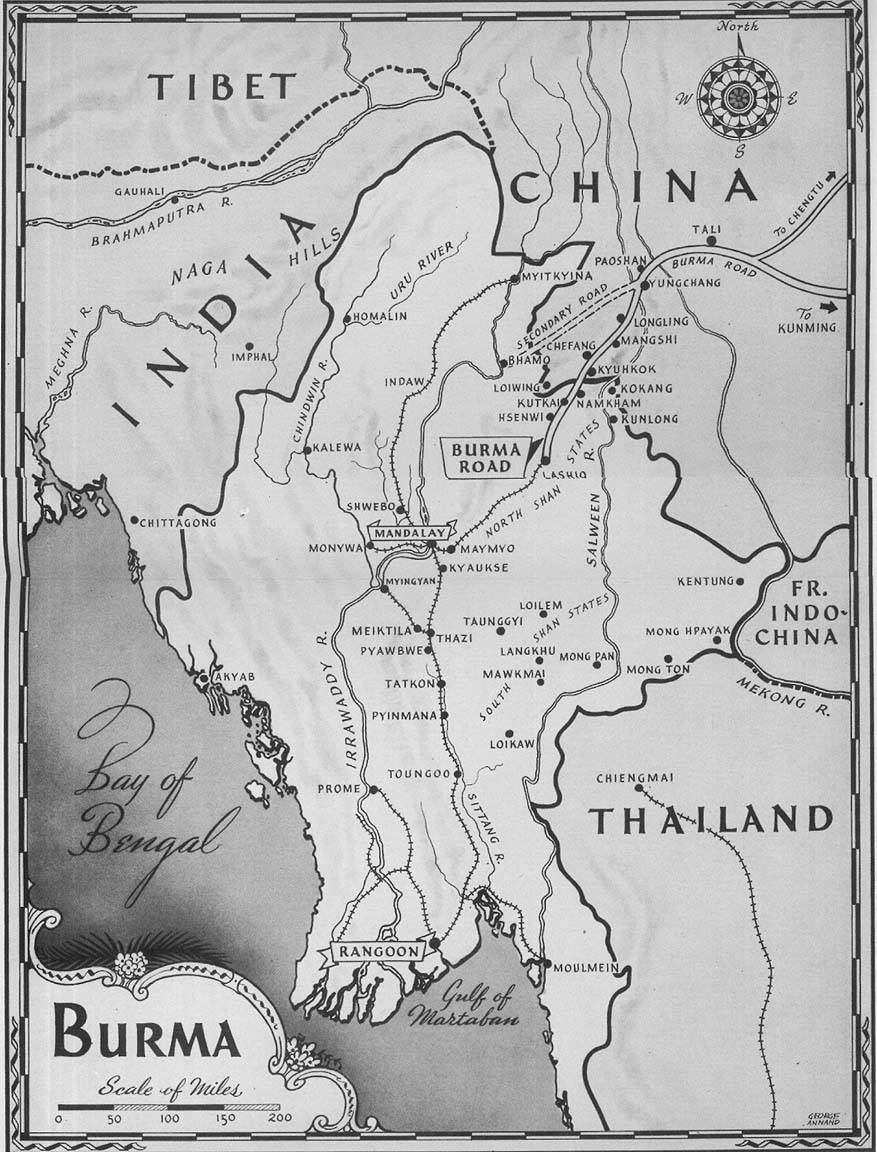
We went by train to Mandalay and then by river steamer three days up the Irrawaddy to Bhamo. How the English do feed! At six o'clock one of the table boys comes banging on your door. You wake up with an angry start, open your door and he stalks in with tea, toast, and marmalade intended to give you sufficient strength to get up two hours later. At nine, before your toast has digested, you sit down to a five-course breakfast. The pain caused by the five courses has not disappeared at one o'clock, when the gong drives you to lunch and you plough through four more courses. At five o'clock there is a big tea to help you live through till dinner at eight or nine. By the third day I had an attack of hiccoughs that lasted five days!
Bhamo is a dirty town. We stayed there only long enough to find mandarin chairs and carriers for Tiny as, of course, she ought not to ride sixty miles on a horse in her condition. The rest of us rode native ponies, and our equipment went up on mules.
We did twelve miles a day, spending the nights in government bungalows. The first day went well. It was all level plain, and the mules, the carriers, and our ponies stayed together in one large caravan. The second day was a long, steep climb. Knowing nothing about the Chinese, I was quite happy as our ponies took the lead. Tiny, in the meanwhile, was having her troubles. Our son was turning somersaults internally and our daughter was turning handflips externally. Leslie's antics constantly shifted the balance of the load and hurt the shoulders of the three Chinese carriers terribly. The Chinese cursed and swore, and Chinese is a wonderful language! They turned so sharply round the corners that though they all three had their feet on the road, Tiny was swung a yard out over the precipice. Then, suddenly, they set Tiny down in the middle of the virgin jungle and all three men disappeared to have a three-hour siesta with their opium pipes. It was the first time Tiny had been through Kachin country, and, until you know the Kachins, their fierceness terrifies you more than the tigers and leopards that howled around Tiny that day. Finally, when we were just preparing to send out a search party, she arrived in camp half dead from fright.
On the fourth day we crossed the great seven-mile-wide Shweli River plain and passed through Namkham Town up the hundred-foot climb to the Shan compound on the right and the Kachin compound on the left. Our hearts were pounding. What sort of setup were we going to find in this place where we were to spend twenty years? The hospital was a rotten wooden building with twenty wooden beds bare of all furnishings. The floor was stained with blood and pus and medicine, and was so rotten you had to step carefully not to break through. Nurses have, since then, scrubbed that floor so thoroughly and so often that the boards are about half as thick as when they were nailed down; yet the stains are still there, for the jungle wood is as porous as a sponge. The walls were covered with large red splashes of the saliva of betel-nut chewers. All the window ledges were covered with nasal secreta which the patients blow on their fingers and then carefully wipe off on the nearest projection.
There was one patient with a leg ulcer.
There was plenty of good will for Dr. Harper to turn over, but what is good will without patients? Yet if there was no medical work to do I could occupy my time elsewhere, for I had four grade schools, one silk-weaving school, one mulberry garden in which to raise silkworms, and one Shan Christian village to keep in order.
That night Marion and I broke down and sobbed in each other's arms.
The next morning we set our teeth and decided that if Namkham wasn't what we wanted it to be, we would get off to an early start and do something about it. I found a Karen preacher chap who spoke English and Shan well, and made him sit with me all day long and help me teach myself Shan. Poor Tiny never had any luck. You can't study Shan with a baby making havoc of your insides. Besides, until she married me, the poor girl had never been farther out of Illinois than that one corner of Wisconsin where we met. No American, unless he lives in the foreign quarters of our big cities, realizes there can really be such a stupid thing as a foreign language.
I got all the breaks. I had spoken Karen before I spoke English and had learned quite a few words of Burmese as a boy in school. Shan, though it had five different tones in which each word could be spoken---each tone with a different meaning---was quite easy for me. At the end of three months I preached my first Shan sermon. That was the worst sermon I ever heard preached in any language. You have to sing Shan, not speak it, and preferably your mouth should be full of betel nut as you sing. I persisted in singing my sermon in the wrong key!
Take the one word hsu. If you say it with an even sound it means "a tiger." If you say it gruffly, down in your belly, it means "straight." When you cut the word off sharp with an axe it means "coat." Sung on high C for a couple of measures it means "happy," and high C staccato means "buy."
Still, I thought I was pretty good. It was time now to kill two birds with one stone: give the accepted evangelistic type of missionary work a fair trial, and, incidentally, advertise Johns Hopkins. I gathered together a gospel team, loaded a mule with medicines, and started off on tour. At each village we called on the headman. He had to admit us, poor fellow, for I was white. When we announced free medicine for all sick, the villagers crowded in. It was too good to miss. We gave each patient just enough of the right medicine to make him want more. One patient didn't want more. He had pylorospasm and I had no belladonna, so I gave him three tablets of pure atropine and told him to take one after every meal and report to me how he felt the next day. He reported in great disgust. He had decided to hurry the cure by taking all three of those tiny tablets at once. His pylorospasm had been cured, but he hadn't been able to spit all day, no matter how much betel nut he chewed. He would, he said, like to have his spit and his pylorospasm back again!
After medicines were distributed, one of the preachers got up and started preaching; whereat, with one accord, everyone got up and went out.
We tried passing out tracts. That went over big. They wanted extra copies for the folks back home! Now we were getting somewhere at last! Or at least I thought so, until I saw them using the pages of the tracts to roll their huge cheroots. Smoking the gospel seemed to me a funny way to convert a man.
My luck was with me again, though, on that trip. A man came to me with tuberculous lungs. I went over him carefully and told him I was sorry, I couldn't do a thing for him. With those lungs he couldn't live more than a year. One year later, to a day, he died, and my reputation among the Shans was made!
Soon after that tour the Kachins threw a huge convention in their mission compound across the street. They had heard of the new doctor, so as soon as they had registered they came over to put me to the test. One man had a huge adenomatous goiter. "You'll have to have the thing cut out," I said, and nearly fainted when he replied, "All right, go ahead."
I ran up to the house.
"Tiny," I called, 'I've got an operation to do. A goiter as big as a grapefruit. Will you give the anesthetic for me? I'll tell you what to do."
Tiny agreed. I got out my pressure cooker and sterilized some towels. The wastebasket instruments were put on to boil. Tiny got the chloroform bottle and started to pour. Then I began to cut; cut and tie, cut and tie. That's all there is to surgery. I cut darn near everything that man had in his neck before I got the goiter out. Then I sewed up his ribbon muscles and skin and sat down beside him to wait. When he was fully conscious I said, "Listen, fellow, I want you to promise me to lie flat on your back for several days. If you try to sit up your neck's going to fall apart. Understand?"
Yes, he understood. He would be a good boy.
Much relieved that he had not died on the table, I went up to breakfast. When I came down, half an hour later, he was already sitting up in bed.
The next morning I was called for an obstetrical case the other side of the river. As I rode up the street that afternoon, on my return, I saw the Kachin convention was having a feast out on the grass. Mr. Sword, the Kachin missionary, waved to me to come and join them. While I was waiting to be served, I looked around and saw a funny apparition. A Kachin man was standing near, dressed in a most extraordinary manner. As Kipling says, "Nothin' much before, an' rather less than 'arf o' that be'ind." He had a bandage around his neck. I looked again. Yes, there was my goiter patient! He had smelled the pork curry and had come across the street to get it. And yet he couldn't die!
This was the first time in northern Burma and the Shan States that a goiter had been successfully removed. People came in willing to take a chance at other operations. I remember a few key cases that opened up whole districts to a confidence in us. There was a cancer of the breast that had already reached the cauliflower stage but was not yet fastened irremovably to the chest wall. She was from Momeik State, down toward the Ruby Mines at Mogok. For years she spread the news of how her breast had been removed and skin from her leg grafted onto her bare chest in sheets! There was a woman with a sarcoma of the orbit pushing her eyeball way out of her head. We removed the eyeball and the tumor, and, until last year, she was still sending patients to us. A rich Chinese came down from Tengyueh, capital of Western Yünnan. He had been inexpertly operated on for amebic abscess of the liver, and the fistula had never closed. He wanted another operation, but we cured him with injections of emetine and irrigations of quinine and salvarsan. A high-class Kachin woman of wide influence had had one girl baby followed by several abortions, and wanted a boy badly. We removed a dermoid cyst of the ovary and a year later she did have a boy.
In lots of these cases we had the breaks. I had not had more than a minimum variety of operations on which to acquire experience under guidance in America, and I looked forward with dread to every new operation I had to do. But I never had any overwhelming love for a quitter. When a new operation needed to be done, I got out my books and studied every detail. Then I was profusely sick, went to bed on it, and the next morning, still nauseated, started operating. Somehow or other, the first three operations of each variety were more or less uncomplicated and the patients got along well. After that---God help me! But by that time I could feel confident that the reason the patient died was not all my fault, and I could continue trying to save lives.
Tiny is quite annoyed at the way I operate. She says that all through my operations I am either praying out loud, singing, or swearing. She is wrong. They are all three just my peculiar way of praying.
In medicine, also, we had the breaks. I was called once to see the sawbwa of Chefang State in China who was "dying" of malaria. Chefang is now just a short trip by car on the Burma Road, but then it took me three days through mud up to the ponies' bellies. When I got there the prince had just about got control of his fever; but I gave him an intravenous injection of quinine and then, when all his lords and ladies gave me the credit for a marvelous cure, I just kept my mouth shut and smiled my gratitude; and patients began to pour in from Chefang State.
The same thing happened with the sawbwa of Mangshi, still farther north in China. He was dying of amebic dysentery, but a few injections of emetine followed by stovarsol tablets, and the patients began to come in droves six days by foot from Mangshi.
These Shan sawbwas are what Maurice Collis calls "Lords of the Sunset" in his book of that name. The Shan title, Saohpa, literally means "Lord of the sky or universe." In Burmese, this Shan title sounds like a very filthy female anatomical cuss word, so they smooth it out to sawbwa. In England these sawbwas would be dukes, earls, or baronets, according to the size of their respective states. Mangshi would be a duke, Che-fang an earl, Hsenwi, in whose state Namkham lies, Kengtung, Hsipaw, Momeik---these would be dukes. Tawngpeng, Yawngwhe, Lawksawk (whose grand-daughter Louise is) would be earls. Wan yin, whose daughter Pearl is, and Hopong would be baronets. In the Shan States of Burma, the sawbwas are chiefs, but their work is supervised by British superintendents and assistant superintendents who are responsible directly to the governor and Defense Department of Burma and not to the Burmese congress.
A year later, when we had developed the hospital to a point where patients were really coming for treatment, I received a letter. Dr. Harper, the writer said, would like to come back for another term at Namkham, so he was sure it was "God's Will" that I should move to Kengtung. How about it? I replied that it was the general consensus last year that it was "God's Will" that I should go to Namkham, and I was sure God didn't change his will so frequently---and I stayed on in Namkham!
WITH SURGERY in the offing it was immediately apparent that we must have nurses. The hospital staff consisted of Tiny and myself, a Karen doctor, and a girl who had had a year of training in Rangoon. Our milkman's wife came running to me one morning to ask me to visit her husband who was sick with malaria. I rode out to their village on my pony and found him very seriously ill. He needed hospitalization. His wife and I managed to get him into my saddle, and, she propping him up on one side and I on the other, we transported him to the hospital without his falling off the pony. I put him to bed and gave him fifteen grains of quinine, for I believed in large doses in those days. My "nurse" was nowhere in evidence. Then I went home for dinner. When I came back an hour later I discovered to my horror that not only had my nurse come in and, seeing a fever case, given him ten grains of quinine, but my assistant doctor had turned up and given him fifteen grains more. The patient almost died of quinine poisoning, but it cured his fever!
We decided then and there that we would train our own nurses. We began with a Shan and a Kachin girl. The Shan girl was the daughter of the chief torture expert of the Chefang sawbwa. Mr. Sword, the Kachin missionary, kindly permitted me to have the Kachin girl, because she had failed all her examinations in school and so was of no further use to him. The language made things difficult. I taught the Shan girl in Shan and she taught the Kachin girl in Burmese! In our operations we had four languages, English, Burmese, Shan, and Kachin, going at once.
Shan girls were hard to obtain, so, after two years, we had one Shan and five Kachin nurses, and my Shan was practically useless. I started to study Kachin but gave it up at once. Kachin is a child's language compared to Shan. It is easy to learn because there isn't anything to it. It has no term for anything important. All the girls, however, had had to study Burmese in school, and Burmese is more expressive even than Shan. So I set myself to learning Burmese by the simple expedient of having the nurses teach me Burmese while I taught them nursing. It worked pretty well except in anatomy where the only names for the genitourinary organs with which the nurses were acquainted were the filthy terms that they had heard used in the bazaars when Burmese women cursed each other. Without realizing it, they were teaching me to be very proficient in profane Burmese.
Tiny had an awful time learning Shan sufficiently well to take the two examinations "required" of missionaries. She had acquired the colloquial quite readily in spite of handicaps, but somehow she always had a baby hanging around, which, plus her extensive duties in the hospital, kept her from getting the book work done. Finally she set her teeth, stayed up late nights, and, a week before John was born, passed both her examinations in Shan simultaneously with great credit. And then we stopped using Shan entirely in the hospital and used Burmese instead! For my part, there was a dearth of textbooks of nursing, and I had to set myself to writing one in Burmese. As it happened, one copy was brought out of Burma after the battle. The rest have been bombed to a pulp by the Japanese, and now the United States Air Force is accounting for any spare copies the Japs missed.
We needed to import a trained nurse from outside to teach general-nursing procedures. That was something I could not do myself, and Tiny had no time to give more than supervision to the class, aside from the fact that she didn't know Burmese. Our first imported nurse was a grand girl, but she was subject to the disease that spoils the work of so many persons in the Far East, namely, homesickness. She used to bathe the patients in her tears as she was caring for them. Our next effort was the nurse wife of an Indian doctor we had for a while. She developed tuberculosis and that was the end of her. Then we tried a couple of American nurses. The first lasted six days and the second six months. Our last effort was the most successful, a very fine Karen nurse named Lucy from Moulmein. She was with us for a long time until she and my Kachin doctor got into a fight, and then we lost both of them.
By this time our training school had reached government standards and obtained government recognition and our first class of English-speaking nurses had passed their state examinations with credit. The top girl in the class was a charming Shan girl named E Hla, with a first-class brain. All through her course her daily recitations and examinations had averaged well over 95 per cent. We put her in as head nurse and she was still head nurse at the time of the evacuation of Burma. During her first three or four years she was not of much assistance in disciplining the younger nurses who had been her schoolmates, but as the years passed her prestige throughout the country was so great that the pupil nurses began to recognize her for her real worth, and she never had to fret about loss of face. Then she married Ai Lun, a boy from a poor Shan family whom I was putting through medical college, and became forthwith an "old woman," with that title's corresponding sharp rise in prestige.
Unless you have seen the jungle races of the Shan States you cannot possibly grasp the problem of training nurses, nor yet appreciate the girls we have trained. We have girls of ten or twelve races continually represented in the school, each with their own language entirely unintelligible to the other race groups. Their only common language is Burmese which they learn in the school---and also in the bazaars---and in the whole history of the school we have had only four pupil nurses who were actually Burmese. The largest race group was Kachin, the next Shan, the next Karen, and then a smattering of other tribes, Hkamti, Padaung, Taungthu, Lahu, Red Karen, Black Karen, Maru, Atsi, Lashi, Pwo, Bghai, and Paku. There were two Indian girls and one Intha. There was one Hkun. The only race we wanted represented, but without success, was the Chinese.
Of them all, the Kachins were the most hopeless-looking when they came for training. The Kachins have a stocky, low-slung chassis, and are, by nature and preference, brigands. They migrated down, the last to come to Burma, from the Chinese-Tibetan divide. With their skill in the use of dabs they were fast chopping themselves southward through the Shans and Burmese, and if the British had not taken over Burma, they would by this time have been unquestioned masters of the country. They are intensely loyal to the British and make the best soldiers of all the Burma races. In the first World War they covered themselves with glory, and did not do so badly in the Battle of Burma, considering their equipment and training. But living in the mountaintops where it is cold and water very difficult to obtain, the Kachin villager never bathes unless someone puts it over on him. That happens three times in his life: once when he is born, once when he is married, and once when he dies. That means that only once in a lifetime does a normal jungle Kachin voluntarily take a bath. A missionary asked a villager once if he ever bathed and he replied, "Yes, teacher, twenty years ago I had a bath and a month later my uncle died. Five years later I had another bath and my cousin died. I haven't dared bathe since!" I never go to a Kachin church service if it can be avoided, for I do not possess a gas mask!
The Kachins of Burma are dying out 1 per cent per year, the chief causes being syphilis and gonorrhea. Syphilis makes Kachin women abort or give birth to dead or dying infants, and gonorrhea seals off their ovarian tubes and makes them sterile. In every normal Kachin home there is one special guestchamber. Kachin custom requires the family to furnish hospitality to all Kachin travelers whether they are acquaintances or not. If the visitor is not "hungry" he sleeps around the fireplace in the main room. If he is "hungry" he goes to the special room and the family have to furnish one of the daughters of the household to entertain him. Kachin boys and girls are supposed to experiment from the age of ten or twelve on. If one of the daughters is a bit shy her mother pushes her out of the house after dinner. A pregnancy makes the girl all the more desirable for marriage as she has proved herself to be not primarily sterile. Any Kachin will marry her happily whether he fathered the child or not.
Dr. Geis, one of the pioneer Kachin missionaries, told me he was convinced there was not a Kachin virgin in the country over ten or twelve years of age. I was horrified, but after a few years of gynecological practice I was sure he was right for that day. Since then a new generation of Christian Kachin girls has grown up. The Kachin missionaries had done a good job ---an extraordinarily good job. The jungle Kachins, of course, heathen Kachins, are the same as before.
There is not nearly so much gonorrhea and syphilis among the Shans. They don't take their sex quite so seriously. Still there is some room for improvement. I was vaccinating some Shan children and the government vaccination register required the entry of the father's name. I asked the young mothers who the fathers were. They giggled.
"Good Lord, we don't know." They change husbands so frequently they cannot quite keep track.
Two Shan women were overheard fighting in the bazaar.
"You are not half as lovely as I am," said one. "You have only had three husbands, while I have had seven."
The people known as Shans were the original inhabitants of southern China. Driven out by the Chinese, they migrated west and south. One branch filtered into Siam and became the Siamese. Those that came into East Burma became the Shans, into West Burma, the Hkamti, and into Assam, the Assamese. They have been civilized for a thousand years. They had kings of their own and contributed at least one dynasty to the throne of Burma. They built walled cities. Subjugated by the Burmese kings, they had Buddhism forced on them, though they retain some of their original spirit worship. The Kachins are pure---pure?---animists. Six hundred years ago a great Burmese monk adapted the Burmese script to Shan needs and they developed a literature of their own. The Kachins have only the English script given them fifty years ago by Baptist missionaries.
Shan women are the most beautiful in Burma. With charming figures, they have lovely light skins and, when healthy, bright rosy cheeks. Chit Sein, one of our nurses, is so gorgeous that the Americans called her "Miss Burma, 1942."
The Karens were in Burma before the Burmese. They are mountain people. Burmese kings subjugated all but those in the Karenni States, and have treated them like scum ever since. They were very religious, with a mythology very close to that of the Jews. When Judson returned from his first furlough in America, he brought with him a group of new missionaries including my two great-grandfathers. Some of these missionaries, including Great-grandfather Vinton, soon turned to the Karens as being much more receptive to Christianity than the Burmese. The missionaries adapted Burmese letters, giving the Karens the most perfect tonal script of any far eastern language. So many hundreds of thousands of Karens have been converted to Christianity since, that Christianity has become their national religion. They have their own Home Mission and Foreign Mission societies. Karen women are by nature kind and gentle, and they constitute the bulk of the nurses in Burma as well as the bulk of children's "nannies." They are completely loyal to the British.
With all these varieties in training, the proper way to maintain discipline was a very serious problem requiring real thought. The ordinary Kachin enjoys being bossed by a man with a loud voice, reinforced by an occasional slap and a couple of kicks. Shans resent even the loud voice, and if you get angry with a Karen girl she becomes positively ill. The only way we could influence them at all was to treat them with respect and affection; affection even when an occasional nurse did not deserve affection, and respect even when it was pretty difficult to respect many, especially in those first days when they were so dirty. A white man or woman "respect" a native girl? Why, in the Buddhist scale, a woman is the next form of life below a male dog! Astonished at being treated with respect they tried all the harder to deserve respect. Receiving affection, they became worthy of affection.
After Dr. Ba Saw, my Karen assistant, had been with me six months, I called him to the office one day and told him how much I admired his manner with the nurses and patients and how pleased I was with the improvement in his surgery and medicine since he had been with me.
"Doctor," he said, very seriously disturbed, "if you praise me like that you will make me go to the dogs."
"No," I replied, "flattery of a person who is unworthy of praise will, it is true, spoil him; but a man who deserves the praise becomes more humble, just as you have become, and tries harder to give satisfaction."
And the nurses did try. Bathed and bathed and bathed---until they were as clean and sweet a group of girls as you could find in any country. On the march out of Burma behind General Stilwell, all we Americans could do when we reached camp was to spread out our blankets and drop down. The nurses, on the other hand, looked for water, bathed, washed out their own and our clothes, dressed our sore feet, and then helped Tun Shein serve up our food.
First, bathing all day long. Then they tried a bit of powder to take the shine off their faces. One of the girls got up her courage and bought some rouge. They decided that was fine. Then someone appeared with a lipstick and overdid the business badly. Some of the others bought one and showed her how ladies of taste did those things. When American women appeared at the Loiwing airplane factory with their nails painted in the most extraordinary colors, the nurses voted against it---until they found some mild, pink fingernail polish. Where do they get this taste? From their jungle ancestors? God knows.
Teaching them nursing is not very simple. Only a few of them have very quick minds. But in all the years only one girl failed her government examination. The process consists in not allowing them to fail. If an occasional probationer simply has no brain, we let her go early. The rest, no matter how stupid they are originally, are taught and taught until they finally understand, no matter how many extra hours the old man has to spend teaching them. Those later years we began to understand their difficulties. Western medicine is completely beyond the comprehension of these girls. Unlike Americans they do not grow up in an atmosphere where modern medical facts and ideas are overheard daily and seen in articles in the press. Medical terms are never heard. Any medical ideas they have acquired during their youth are all wrong, the vaporizings of native quacks. The courses taught them on government schedule, they cannot grasp in the way necessary to satisfy you.
But with three and four years under you, living in hospital, seeing thousands of cases, they pick up so much new vocabulary as to amount almost to a new language. Now, during their last year, we teach seniors---very, very rapidly---their course over again as if they were brand new probationers. This time they really comprehend.
One day, as they were doing their ward work together, Captain Webb was teasing Kyang Tswi by giving her some quiz questions.
"What do you know, if anything, about placenta previa?" he asked.
"Well," answered Kyang Tswi, "there are three kinds of placenta previa, central, marginal, and partial . . ." and forthwith gave him a fifteen-minute harangue on the subject. She hadn't had a peep at a textbook for eight months.
If nothing else made for good discipline, the fact that they knew, from years of observation, that we were determined to succeed in making good nurses out of them certainly made them co-operate.
Their adaptability is remarkable. When we reached India after the Battle of Burma, I brought Lieng Sing, our Chinese college boy from Singapore and Rangoon, and five nurses with me to Calcutta to purchase new equipment for the crowd. On the train we had to have lunch in the dining car under the stare of British officers. I led them in in fear and trembling. The array of silverware at such a meal is awe-inspiring; I had often had trouble myself being sure just which implement to use. But the only error that appeared was committed by the girl who had grown up in Rangoon. The rest, Kachin, Karen, Shan, from the wild jungles, did everything perfectly. I couldn't understand it till I saw they were watching me out of the corners of their eyes.
We went to a movie. Unconsciously Koi crossed her legs, bringing her foot within the range of vision of a certain officer in front of her. He thought this would be easy, grasped her foot and began climbing slowly up her leg. Koi tried gently to release her foot. He held tight. She tried again, using more strength, but without success. And then---she kicked him!
On our way home we had to hurry so I wouldn't miss my train. Koi and Hla Sein walked ahead, then came Esther and Lieng Sing, while Little Bawk, Big Bawk, and I brought up the rear. A soldier who looked like a Gurkha saw the first two girls and asked them if they were Burmese. They walked on. He fell in step and did his best to start an acquaintance. They continued to chat unconcernedly together. He gave up and turned back, coming face to face with Esther.
"Why, Esther, what are you doing in India? When did you last see your folks?"
Esther, recognizing an old Bhamo schoolmate, stopped to talk. Lieng Sing walked on out of earshot, stopped and waited for Esther to finish her conversation before escorting her home. The Bawks and I walked on by, convinced that these "uncivilized," "jungle" girls could take care of themselves even in one of the largest and most wicked cities of the world, in a country completely foreign to themselves. Where did they learn these things? God knows.
We had orders to push on from Assam to "somewhere in India," and we traveled by troop train. There were four nurses in a compartment. At three in the morning, as we were drawing into a station, a soldier climbed from his compartment through their open window. The nurse in the nearest berth screamed as he stepped in on her, and the other three girls joined her in throwing the soldier out of the window while the train was still moving! We never heard what happened to the soldier.
One thing I learned from sore experience. You could not hope to handle these nurses, no matter of what race, in groups. No argument, no matter how sound, is ever effective with them as long as they are permitted to gang up on you. Singly, and handled with affection and respect, they see the point of your argument at once, and respond. Handled as individuals and with respect and affection, we can get twelve and fourteen hours of very efficient work per day out of these girls, and they sing and smile and joke as they work. And work they will until they get tuberculosis or drop from simple overfatigue. But let them gang up, even with only one other person, and you can't argue with them at all. This has been proved numberless times. In a gang they give each other courage to resist the "old man," as they used to call me. All we ever needed to do was to separate the different members of the gang, give them jobs in different places, call them in and explain the situation to them one by one, and the affair was over. It takes courage to do wrong, and you get that courage artificially through some fellow worker who wants to do the same wrong thing.
In a hospital it is as important as in any army that orders be obeyed. Our orders were obeyed---or else! But there is much more co-operation if the reason for the order is explained, when it is not in itself apparent. Also, it is much easier to lead than to drive. That is where human beings differ from horses. In no Indian or Burmese hospital do the nurses do any dirty work. There are special castes to do individual jobs. It makes the hospital bulky with lazy personnel. It is costly. It makes it hard for the patient to get real service, unless he has plenty of money for "backsheesh." We were determined that any nurses we trained should be willing to do anything needed, no matter how foul. All I had to do was do the dirty job myself. Lose face? A big man cannot lose face. It is the petty person who has to fret about losing face. I can open up the manhole in our sewer system and clean it out with my bare hands in front of a crowd and not lose face thereby. In fact, the crowd will turn in and help me clean it out so they won't lose face by doing nothing when the old man is busy.
The first order any nurse received when she entered training was that she must be gentle. Any lack of gentleness in doing dressings or giving nursing treatment of any sort is punished drastically. If nurses don't care what happens to their patients when they first enter training they soon throw it off. Once a patient with cerebral malaria walked out of the ward, while the nurse's back was turned, and disappeared. We searched all over the neighborhood without success. Twenty-four hours later a party of soldiers discovered him lying in a marsh, half under water. They brought him back to the ward, and his temperature went steadily up till, at dawn, it reached 107° and he died. When the night-duty nurses came off, two of them were sobbing.
"What are you crying about now?" I asked.
"We tried so hard to keep that patient of yours alive, and all the time he was dying the other patients stood around and made fun of him. Nobody cared about his dying except us!"
When the night girls took over, one night, they found Thelma had written this on the night-order sheet: "Please take care of these particular patients [bed numbers of serious cases followed]. They are all my honeys, so do all you can for them."
We had some strange doctors working with the unit.
Another nurse came to me, her cheeks wet with tears. "Daddy, Doctor Blank won't give me any orders for Bed No. X. He says the patient is going to die and wants me to let him die---and I don't want to let him die."
"O.K., see what digitalin and a Namkham intravenous glucose will do for him."
The patient recovered.
Nursing Chinese patients is about as difficult a job as a nurse can possibly be asked to handle. They simply won't take their medicine. Hla Sein solved the problem. I was walking by her ward when I heard her singing at the top of her voice. I thought she must be mad so I peeped in the door. She had her bottle of quinine solution in one hand and her dram glass in the other. All the malaria patients were lying at attention. She stepped up to one after another, sang him a verse until he started to laugh, and when he had his mouth wide open poured in the bitter stuff. Her patients acted as though it was Jove's nectar she was feeding them.
The girls are so tiny. About five feet tall, they weigh from eighty to a hundred and ten pounds. One of them had such small feet that when she bought shoes she had to buy them in children's sizes. But you should see them heave their patients around, move them from stretcher to operating table and back again. They stood the long, hard tramp out of Burma better than the Americans, and got through into India in much better physical condition.
The United States Army speaks of these girls of ours as Seagrave's Burmese nurses. The nurses are not Burmese. Only Than Shwe is Burmese. But I don't mind. The other girls were born Karen, Shan, Kachin, Taungthu, and so forth, but we wouldn't tolerate their remaining Taungthu, Kachin, Shan, and Karen. We wouldn't tolerate any race differentiation. They had to be bigger than their race or we had no further use for them. At first Kachin would clique with Kachin and Shan with Shan. The old man didn't approve. He fought them tooth and nail. The head nurses would report errors of conduct of girls of other races, not of their own. The old man would disgrace himself by getting downright angry. An occasional Karen would start chumming with a Shan, a Kachin with a Taungthu. The old man would praise them from the pulpit on Sunday when it was his turn to preach. Now race has nothing to do with any of them. They are much bigger than their race. Little Bawk and Chit Sein, Kachin and Shan. When Bawk goes off on sick leave Chit Sein mopes around and. gets sick herself. The Shan girl can't live without the Kachin. Koi and Saw Yin, Shan and Karen. Roi Tsai and Lu Lu, Kachin and Karen. Lu Lu thought I didn't approve of her friendship with Roi Tsai, and for months she couldn't work, until the matter was straightened out. Kyang Tswi and Esther, Kachin and Karen. United by a wholehearted decision that our fellow worker Paul Geren was a present-day incarnation of God, they couldn't be separated. If their regard for him were based on sex they would be jealous of each other. No matter what others may think, it isn't a case of sex at all; in their minds he just gets mixed up with their ideas of God--I don't blame them---and it brings them together.
At the boardinghouse where we stayed in Calcutta we met two very respected friends of mine, Dr. and Mrs. Jury, two of the finest old Burma missionaries you could hope to see. I told them that the five nurses were Kachin, Shan, and Karen, and invited them to see if they could tell which was which. If anyone could tell them apart, they should have been able; but they missed every one.
They are bigger than race, bigger than nationalists. What price a solution of this horrible world's difficulties! If Germans were bigger than Germans. If English and Americans and Russians were bigger than Russians, Americans, and English. If there were something bigger than patriotism, bigger than love of country! Would we continue to have these wars? We have no more racial strife among these nurses. We have individual strife when they have not enough work to do, but it is no longer based on race, and is therefore very short-lived.
WITH NURSES to help, we began to take on all sorts of cases. It was to Kachins that we owed our ability to develop surgery. Having lived by the dab they were not afraid of the knife and came to have a most unbalanced admiration for my prowess with that instrument. One day in Bhamo, a Kachin with a gastric ulcer came to me to be examined. When I told him he needed an operation, he took off his shirt, pulled out his gigantic sword, put it into my hand, lay down on the floor and said, "O.K., Doctor, go ahead."
Not having an X-ray in those years, I particularly dreaded orthopedics. I used to escort the patients to the door and say, "My dear fellow, you need an operation, all right, but I don't know how to do it. You'd better run along home and forget about it." And half an hour later he'd be back again.
"Doctor, I want you to operate on me."
"But I don't know how, I tell you; I am afraid you will die."
"That doesn't matter, I won't blame you if I die."
"No, I rather guess you won't. All right, if you don't mind dying I'll do my best to satisfy you!"
I opened my first pus abdomen and put in a rubber-tube drain. When I did the first dressing, the drain had disappeared. I probed around in the man's belly but couldn't find it.
"What are you looking for, Doctor?" asked the patient.
"I'm looking for that rubber tube I stuck in you. It's lost."
"Oh, that thing. Well it was hurting me so I pulled it out and threw it away."
In those days we were so poor I couldn't afford to lose that tube. I couldn't find it in the ward, but on the verandah I was delighted to come across a baby using it for a pacifier.
When I took the dressings off my first hernia case to remove the stitches, I found the patient had anticipated me and had scratched them all out with his fingernails, and the wound was wide open. I began to be profane.
"Doctor, it itched. I had to scratch, didn't I?"
Judson College in the University of Rangoon wanted me to address the student body. I told them that all my appendix cases in those first years had died. In one of the front pews was a young professor who seemed to be very interested in my talk. He sat on the edge of the seat just drinking in my words. At the close he came up and pumped my arm up and down.
"Doctor, that was a wonderful talk. You have done me a great deal of good and given me a lot of comfort; I am to have my appendix out tomorrow."
I like to be a comfort to people!
No appendix case came to me those first years unless the appendix had been ruptured at least a month, and one patient had ruptured his three months before I saw him. Sulfanilamide had not appeared.
Personally, I always wished I could specialize in gynecology. But how can you limit yourself to specializing in any one thing in a country like that? Still we had plenty of gynecological cases to keep life interesting. The medical colleges in Burma and India are alike in that very little gynecology can be studied by male medical students, and the status of gynecological operative work is poor. Women will come to a medical missionary much sooner than to government men. Kachin tendencies toward gonorrhea would keep us supplied when other cases petered out.
Next to gynecology, I would like to be an obstetrician. And what a chance I had to be an obstetrician! No woman, much less her husband, would call me for a normal delivery, in those first days. But when everything went wrong, even the husband would call me. We had a marvelous variety of abnormal obstetrics. When the matter got beyond my depth, I had, as usual, to appeal to Tiny. Tiny took my course in midwifery and started pulling babies. A good teacher is one who can teach his pupils to become better than he is. That's how I know what a good teacher I am. I taught Tiny how to give a chloroform anesthetic, and she now can give a much better one than I can, keep the patient under for four hours without a symptom of chloroform poisoning. I taught her obstetrics, and now she can slip her long, slender fingers up into the fundus, rotate and deliver, when my fist would rupture the uterus at the first try. I always got a laugh when she went to work on a child that wouldn't breathe. The sweat poured from her face. Her temper became brittle. She panted like an exhausted runner, and panted life into the child long after I would have given it up for lost.
The only obstetrical instrument the natives have is the sharp hook. They tear the baby apart with it, rupture the uterus and even rip out half the vagina. But they get the baby out, which to them is the essential point, even if the mother and baby both die. The mother would lose face if she died with the baby still in her.
They carried in a woman with pain down below the appendix region. "She has an extrauterine pregnancy and will have to be operated on at once," I told her employer.
"Nonsense," said he, "who ever heard of a baby growing anywhere else than in the uterus?"
"Well, this one is, and I am going to operate right away."
"Not if I can help it. You have to send for her husband and operate after he gives his permission."
"He lives so far away it will take him two days to get here, and by that time there won't be any woman left to operate on," I said, and started to scrub up.
The employer, with a grim face, insisted on remaining in the operating room so as to have the goods on me if I had missed my diagnosis---remained until, on incising the peritoneum, a couple of pints of clotted blood burst forth, and then he had himself carried out by the nurses quite content, and convinced that babies were sometimes indiscreet in their choice of residence.
My first mastoid case was a charming little Kachin schoolgirl. I had never done a mastoid, but I had an old dry skull in the hospital. I pulled it out and did a mastoid operation on it, and when nothing happened to that patient I operated on the little girl, and she did well. We had many other mastoids. One came to us in a dying condition, the pus having burst through the skin, and he had a large Betzold abscess in the neck---and his ear canal and his mastoid were full of maggots. I opened the abscess, but his condition was so poor I didn't dare to do anything else. I just put him to bed and told the nurses to compel him to eat. But, like all men who are ill, he was very hard to feed. He didn't want eggs or milk or toast or anything else that was good for him. All he was willing to eat was rotten fish and a sour pickle! The nurses had been trained never to waste a cent of hospital money, and they couldn't see the sense of pushing good food down a man who was going to die anyway. So I went out, bought the rotten fish and the sour pickle the fellow wanted, fed it to him myself, and he got well.
My first gastrectomy for cancer of the stomach did well until the patient went home, and then he sent back word that I was a rotten doctor; he couldn't stow away the gigantic amounts of rice that Shans eat twice a day without getting terrible pains. It took two months to persuade him he would have no pains if he would eat smaller amounts several times a day.
Stone in the bladder is very common. My largest weighed sixteen rupees. It had been in the patient's bladder twelve years, ten of which he had spent incapacitated for work.
There was a lot of plastic surgery forced on us. There was a Chinese who had most literally "lost face," a bear having disposed of most of it including one eye, the nose, and the upper lip. A bit of skin was left on the forehead which I used as a pedicle flap to line his new nose. Then I took cartilage from one of his ribs, grafted it in for a support, and finished off his new nose with a caterpillar graft from his chest. It was rather a flat nose, but what better for a Chinese?
Dr. Hoag of Detroit told his Bible class about this case. When he had finished speaking, one of the deacons called out, "Pastor, that is not the first time something 'nosey' has been made out of a rib!"
A woman came in one day with the worst infection of lice I had ever seen. Her hair had millions of them in permanent occupation. They had bitten her on the forehead and nose until she itched so badly she had scratched the front of her head full of sores. Flies had laid their eggs and now her sores were full of maggots. They had eaten into her nose until the cartilaginous part was separating itself from the bone. After we had excised the worst areas and rid her of the maggots, the front of her head had no scalp left. We left pedicles in both temporal regions, moved the scalp from the top of her head forward, grafted skin from her leg on the newly denuded area, so that when she got well she could comb her hair up over the bald spot and hide it very effectively. She came back to me last year with an attack of malaria. This time she had no lice.
I even tried my hand at dentistry, and once I filled one of my own teeth. I had a wisdom tooth that was giving me a lot of trouble and there was no chance to go to Rangoon. So I got out my dental machine and began to grind. I was rather clever at that part of it. I did just like the dentists in the States. You know how they do it. I ground around until I found a place that hurt, and then I ground there a little extra! Then I mixed up the amalgam and pressed the filling home. But somehow, down in the bottom of that cavity I had left a bit of cotton so that when I did finally get down to civilization the whole tooth had to come out. But I filled the tooth anyway.
One of the missionaries in Lower Burma, Dr. Condict, used to pull hundreds of teeth every day. He was a doctor of divinity and not of dentistry. I could not understand why a preacher should pull so many thousands of teeth until I finally got the solution. You put one thumb in the patient's mouth and push down hard on his tongue. You fasten a tooth forceps on one of his large molars. Now you have got him where you want him. He can't talk back and he can't get away and you can preach to him all day long!
And always there were goiters. One was so large it looked like a ham. I had the reputation of being the goiter specialist of Burma. And how I hate goiter surgery. Those huge adenomata would seem to be fed by twenty-five jugular veins, and the walls of so many were so very fragile. I used to be nauseated for every operation. But they would keep referring those confounded cases to me from Rangoon and Monywa, Bassein and Yenangyaung. All our Lower Burma cases were exophthalmic, none of our Shan States cases was. I have never even read of abscessed goiters as large as many we saw. Abscessed adenomata. They seemed unusually common. In most of the cases an emergency incision to remove pus would stop the dyspnea and we could take out the tumor at our leisure. One patient was choking to death as he was carried in. In one case I did not suspect abscess and removed the abscessed tumor intact without the patient turning a hair.
But how can you specialize in anything in a country like that? You cannot do what you want to do and you cannot avoid doing things that you don't want to do. Still I did specialize, and on something new! Wastebasket surgery. Surgery with wastebasket instruments. Orthopedic surgery without an X-ray. Urological surgery without a cystoscope. Surgery without any actual cautery except a stray soldering iron. Surgery without electricity. Medicine without a laboratory, and without medicines, often. Hospitalization without a real hospital or any adequate equipment.
I used to be bitter about it, but now I am rather glad that I had to use wastebasket instruments for so many years, for I have seen what would have happened to me if I had had real tools. I had a Chinese carpenter working for me who had wonderful tools. He had the best saw that money could buy. The result was that when I asked him for a two-foot board he never handed me one from a pile of two-foot boards. He pulled out his saw and sawed off two feet from a fourteen-foot board every time. That is what happens to you when you have good tools. I, on the other hand, have become a very conservative surgeon!
The five most common disease entities in the Shan States are, in sequence, malaria, goiter, amebic dysentery, gonorrhea, and syphilis. Goiter we used to treat with iodine in one form or another if it was of the smooth type, and surgery if it was adenomatous. I had a lot to learn about the other four diseases. With malaria and dysentery I was my own guinea pig, for a doctor in the Shan States cannot possibly avoid those diseases, but I have consistently refused to allow myself to become a guinea pig for gonorrhea and syphilis.
From Assam, across the Chin and Naga Hills, the Northern Shan States and Southern Yünnan, stretch valleys of what the Rockefeller Foundation Malaria Commission men describe as the most perniciously relapsing type of malignant malaria they have encountered anywhere in the world. In the valleys from, say, fifteen hundred to three thousand feet above sea level, the malaria is 97 per cent malignant tertian, 2-1/2 per cent benign tertian, and 1/2 of 1 per cent quartan. That had been my statement before they came to work in the valleys of Southern Yünnan, and their reports confirmed it. Higher or lower the percentages change quickly in favor of the benign tertian. The malignancy is borne out in Chinese history, and Chinese who knew their history dreaded to enter or pass through those valleys. Chinese came in swarms to Burma every November, when the malaria disappeared, and, having found work and made their pile, rushed back to China and its mountains before malaria returned with the rains in May. It was only with the Sino-Japanese War that Chinese came into Burma and remained there during the rains. Shans have resistance to malaria, acquired by the survival of the fittest. Kachins need no immunity, for they live in the mountaintops above malignant malaria levels. The Chinese have no resistance to malaria at all. Before they came to stay, we had very rarely a patient with algid or cerebral malaria or with blackwater fever. After the Chinese came, we had hundreds of cases, and, with the increased virulence of the plasmodium as it passed through the nonresistant bodies of the Chinese, these especially malignant forms of the disease became more common among the Shans and Kachins.
Some of these cerebral malaria cases were unconscious for six weeks before they threw it off. One patient had a mania for breaking windows. After he had broken every single windowpane in his room he felt satisfied and settled down to get well. After an attack of cerebral malaria the English government officers were required to take two years' sick leave before returning to duty. I had a nurse from Lower Burma who was quite superstitious. When she was ready to start north for training she consulted a Buddhist monk who was a reputed soothsayer. "I see your footprints going to Namkham," he said, "but I see none returning." The nurse translated that to mean that she was going to die in Namkham. She got malaria.
We began treatment at once which, with any other case, would have cured her. But she developed cerebral symptoms, and her mania was that she was going to die; and die she did, forthwith.
Of all the forms of malignant malaria, the algid is the worst. The patient with an overwhelming infection of plasmodia is icy to the touch. I have never cured one. I thought I was going to cure one once because large injections of intravenous glucose seemed to have started a reaction, but he died anyway. Chinese are very fond of this type.
Blackwater fever seems to occur only in special circumstances: patients with a special type of kidney, with very slightly or not at all enlarged spleens. It usually occurs in a person who has had chronic malaria for a long time; but I have seen blackwater fever occur in patients with their first attack of malaria. The mortality in the books is very high, but with us it has been very low. This was due to early diagnosis. There is something---what is it, a smell?---about a blackwater fever case. When you see, or smell, that something, a guaiac test is made at once on the urine. If there is no urine available, you assume that it is blackwater fever, for there is marked oliguria in blackwater fever. You immediately treat the case as blackwater fever with atabrine and neosalvarsan and avoid quinine as you would the plague. If you start treatment for blackwater fever before the urine has become black, percentages of cure are high, but if you don't suspect the disease before the urine is black, you cure very few.
As a missionary I was a most unorthodox pain in the neck. As a doctor also I was decidedly unorthodox. A good doctor frequently is the one who gets his diagnosis, no matter what has happened to the patient in the meantime. In a country where 97 per cent of the fevers are malaria, and malignant malaria at that, and where 99 per cent of the dysenteries are amebic, a good doctor will give no quinine or atabrine to the fever case or emetine to the dysentery unless and until the laboratory turns in a positive report for plasmodium and/or amebae. The fact that only one out of ten laboratory men in the country is capable of seeing malaria parasites and amebae makes no difference. If the parasites are not seen, the malaria patient is treated with aspirin and the amebic dysentery with saline cathartics. If the patient dies he is being most unco-operative. Even when the report from the laboratory is positive, treatment has been delayed for anything from twenty-four to seventy-two hours. I would personally rather treat the patient according to his smell and get him well.
During the past ten years the orthodox treatment of malaria has varied a good deal. As each treatment came out, it was, by hypothesis, perfect. You wrote out the order on the chart and said good-by to the patient, sometimes forever! You never adapted your treatment to the special case. If your patient died, it was of course his own fault. He was trying to be nasty. Any doctor who used quinine during the atabrine epidemic was just being old-fashioned. Our routine treatment had to be based on the fact that atabrine was either not procurable at all, or cost too much. But the most important point in our routine treatment is that it must not be routine. You feel your way along with the individual case and use quinine, atabrine, and especially that most divine drug, neosalvarsan, as the patient has need. Neosalvarsan has as many uses, almost, as bamboo. It will cure syphilis. Intravenously injected and unassisted it will cure a good many malarias and blackwater fevers. It is the best stimulant of the bone marrow ever produced for tropical anemias. Put it into the rectum and it will even cure amebic dysentery. It brings down the temperature of relapsing fever in twenty-four hours. But no matter what drug you may use, you cannot cure malaria in a white man without putting him to bed. That is why I never cure myself of malaria even with my own treatment. I can't catch myself still long enough to tie my hands and legs and put myself to bed. If you put your patient to bed you can cure him in about three days by giving him one intravenous injection of five grains of quinine once a day without other drugs, providing you make no mistake in the time you give the injection.
Atabrine, according to its backers, will never need to be supervised. But even the original German atabrine will cause an occasional psychosis of the manic-depressive type, and with the English "atabrines" these psychoses are common.
The malaria belt mentioned above must also be the fatherland of all the amebae. There is very little bacillary dysentery indeed. You can ignore figures to the contrary. It is customary in the hospitals of the East to call all dysenteries bacillary when the laboratory technician turns in a negative report for amebae. But as above said, the number of laboratory men in Burma who can see an ameba, even when present, can be counted on the fingers of your hands. It was not until "Big Brother" Chesley joined us that an "ameba negative" report from the lab meant a thing to me. If Chesley cannot see an ameba, the ameba simply does not exist.
If, in a strange jungle village, you want to know where the village latrine is, you only need to pick up a stick and the pigs will lead you there. Every stream and every well is full of amebae.
The medical examiner of the Mission Board in New York once said, "If Seagrave were a good doctor, he would not allow himself to get infected with malaria and dysentery." That is quite correct. If I had been a good doctor, missionary doctor, I would have climbed under the mosquito net at 6:00 P.M. every night and stayed there and I would have boiled all my drinking water myself. I certainly would not have let my cook "boil" it for me, nor would I ever have answered those numberless emergency calls at night to villages near and far. I would have let the crazy fools go ahead and die unassisted.
With these two diseases the most common everywhere, the nurses became very proficient with the hypodermic and intravenous syringes, much to the distress of the medical profession in Burma, who wanted these money-making procedures in their own hands. When nurses needed practice, they practiced on me. I had a government official visiting me one day. As we left the offices and started down the stairs, the nurse came up with my emetine. I rolled up my sleeves and she stuck it in.
"Good Lord! You don't let a nurse give you a hypodermic, do you?" I certainly do. I would rather any one of our nurses gave me an intravenous quinine than any doctor. Tiny and our son, John, went to Rangoon alone once, and John developed dysentery; so she took him to a doctor there. The doctor put the syringe together, broke off the neck of the emetine ampoule, sucked up the solution and wiped the needle on his thumb.
On Tiny's insistence he condescended to put the needle into alcohol a second. Then Tiny wiped John's arm with alcohol to make sure it would be done, but the doctor wiped off the alcohol with his bare hand and plunged the needle in before Tiny could object. Our first-year girls can do better than that.
Not long ago a new doctor who was working with us gave an order for the intravenous nurse to prepare a solution of glucose for intravenous injection to one of our patients. The girl took the apparatus over to the ward. The doctor tried, and he tried, and he tried, and could not get the needle in.
"Hold everything," he said, "and I'll go over and call Captain Grindlay."
Just then I happened in on my rounds. The nurse told me about the trouble. She didn't think the doctor wanted her to give the injection, he might be prejudiced against nurses.
"O.K., I'll have a try," I said, and ruined a couple more veins. "Here take this thing away from me and put it in yourself," I said.
There was only one vein available, about half the size of those we doctors had been playing with. The nurse took the needle, bent over and got it in the first time. The same thing has happened three other times.
There is not much tuberculosis among Shans. They live in comparatively bright and open houses under better circumstances than the other tribes. Kachins have less-open houses, full of smoke, and they sleep with their heads buried in blankets. Still, as long as they remain where they belong, in the mountaintops, tuberculosis is not too common. It is when they come down into the plains that they get tuberculosis readily. The Chinese have the largest proportion of tuberculosis. Yunnanese live in mud-brick houses with practically no air and they are very unsanitary. For their tuberculosis their only treatment is opium. Opium will stop the cough temporarily, and sometimes permanently!
The most expensive department of our hospital was the pediatrics department. Milk costs much more for one baby per day than rice and vegetables would cost for three adults. But there were a lot of babies whose mothers had died soon after birth, and the babies would die too if we did not take them in. There were a few abandoned babies also, usually twins. Orientals detest twins, and I know of several instances where newborn twins were left to die unfed. The Siamese also do not like them, so that the twins there developed a new variety, Siamese twins, where they stuck together for safety!
The year we reached Burma, the road that later became the Burma portion of the famous Burma Road had just been completed from Lashio to Namkham. It was just a mud road and was only usable six months of the year, and not always then. The bridges were all of bamboo and had to be replaced after every rainy season. Bamboo makes quite nice bridges. You break through them very frequently, but they very seldom collapse en masse under you. I had that happen only once. Usually you jack yourself out of the hole, throw some bamboos in and take off again. During the first year we had no car. The second year we got a second-hand Harley-Davidson motorcycle with a sidecar. It simply could not manage those awful hills even without the sidecar. Just then the government announced compulsory physical exams for all schoolchildren in Burma, the examiner to be paid fifteen cents for every pupil.
I examined so many thousands during my vacations that we managed to buy a Model T. Still most of our traveling had to be done on foot or on tiny native ponies. On a good many trips I could cover double distance; I would ride fifteen miles, leave the horse, and walk another fifteen before dark. The first time I did this I arrived in Wurraboom, halfway to Bhamo, at night, without food or bedding. The local teacher's wife, one of the most attractive Kachin women I have ever met, saw me and brought over some lovely clean blankets and sheets, killed the fatted chicken, and served me up a nice dinner with her one-year-old daughter strapped on her back. That daughter was Myi Tung Bawk, later known as M. T. Bawk, or "Big Bawk." Sixteen years later, her mother having in the meanwhile died of tuberculosis, Big Bawk came to us for training.
That same year, the wife of the most attractive Kachin man I have ever met had a daughter born by the breech. They called her Bawk, too: Maru Bawk, alias "Little Bawk." When she was seventeen, she also entered the nursing school. Bawk is the given name, or rather number. Big Bawk was number-two girl of the Myi Tung family, and Little Bawk was number-two girl of the Maru family. I used to see Big Bawk occasionally on my trips to Bhamo. I saw Little Bawk all the time. She went to school across the street and used to play around with Ruth Sword. They had been playing with my eldest son on the morning of the day he was drowned.
A couple of years later a Shan family moved down from China and settled in our Christian village. They had a skinny little daughter named Koi: "the last one." I can always get a rise out of Koi, who is now the head nurse of our unit, by asking her how her father and mother knew she was going to be the last one!
 |
 |
 |
|
|
||
 |
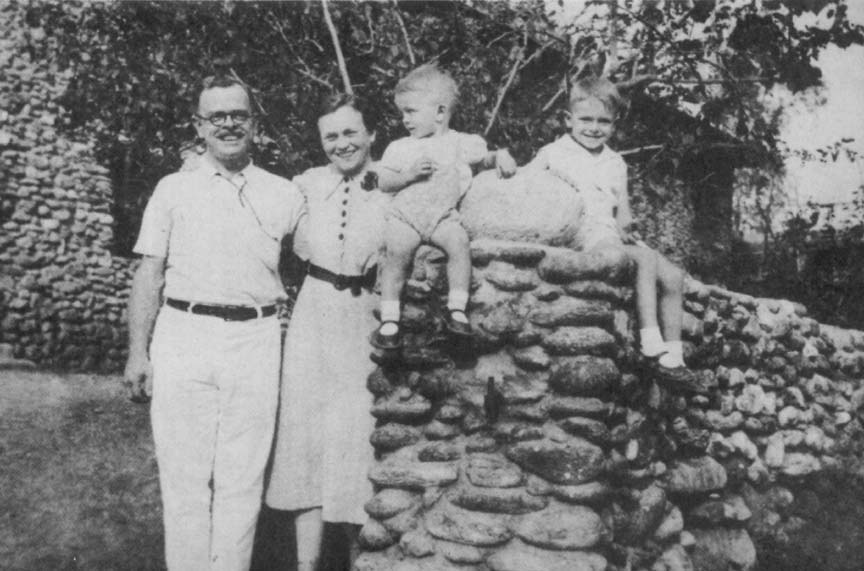 Dr. and Mrs. Seagrave with Their Two Young Boys [W. D. Sutton] |
She did all her school work in our school. She has an astonishing brain. I asked her to let me look at her notes on one of my lectures once. No one knows better than myself how difficult it is to lecture in a foreign language without messing up idioms and failing to connote correctly one's real meaning. In her notes Koi had not only taken down every word I had said, but, at full speed, had changed to correct Burmese idioms and had changed a word here and there so as to get the proper connotation that I had desired. When we abandoned all our possessions in the jungle for the trek out of Burma, Koi abandoned even her last blanket, for fear she would not be able to keep up with General Stilwell, but she carted that notebook along.
When Koi comes to talk to me she can do it in either Burmese or Shan, and sometimes she even does it in English. I can never be sure just what language she is going to use. When we were at our busiest behind the Chinese Army in the Toungoo battle, her report consisted of two words which could have been either Burmese or Shan, though with meanings hundreds of miles apart. A glint came in my eye.
"Koi," I said, "what language are you speaking to me in? Shan?"
She stopped just one second to think what her word would mean if it were Shan, and then she picked up a broom and chased me out of the operating room!
Her own name gives her a lot of trouble, and the rest of us a lot of laughs. The Americans always call her "Hkoi," which, in Shan, is a very dirty word. Finally I took pity on her and told the Americans to call her Goi, which is neither Shan nor Burmese.
For twenty years our hospital had to fight to keep out of the wastebasket. The American Baptist Foreign Mission did not believe in any more large hospitals than they could possibly avoid. In Burma they believed in schools and had a number of them everywhere. For the rest they wanted the work to be evangelistic. Not only did they not encourage you to develop a large hospital practice but they encouraged you not to. One very able doctor, son of a Burma missionary, would have been in Burma had he not been told that he must promise not to develop a large hospital practice. He could have a dispensary or two, but that was all. My hospital appropriation from mission funds when I had thirty in-patients at a time was six hundred dollars. When I had two hundred in-patients it was twelve hundred dollars a year. We received also a government grant which was one thousand dollars a year from the thirty-bed stage, and was not raised until we were well over the hundred mark.
But I lived among those people and saw their misery. The nearest hospitals that ever did any surgery were at Bhamo, sixty miles west, Mandalay and Maymyo, three hundred miles southwest with jungle paths in between, Lashio, a hundred and twenty miles south, and Kunming, about six hundred miles northeast. I could understand no mission work that cared not to alleviate in a really practical way the ghastly physical misery of the people. The Student Volunteer Group for Foreign Missions had the motto, "The Evangelization of the World in This Generation." Even if you have hundreds of thousands of missionaries you can't really evangelize except by consistent work for at least three generations. The Americans aren't thoroughly evangelized yet after two thousand years. If they were, they couldn't stand the pain of the world. All in all, with my eccentric ideas of mission work, I was a thorn in the side of the Burma mission for years.
If evangelistic missionaries suffered half as much at failure to "cure" a man's "soul" as a doctor does when he can't cure the man's body, we might get somewhere. The old-time missionaries really did. They spoke the native languages like the natives. Their people's joys were their joys, and their sorrows theirs also. If the missionaries were going to have some fun they took their people along to share that fun with them. Nowadays it is the rare missionary that can speak the native languages intelligibly. When he has put in the correct number of hours of work he goes home and has his fun with other white people.
I used to be sensitive to the very general low opinion of Americans for missionaries. But how can we blame ordinary Americans for their low opinion when the pastors of the churches that send out those missionaries have a still lower opinion of them? I had been making a speech in the large Baptist Church at Ann Arbor, Michigan. The pastor liked my talk so well he felt like doing me a favor, and took me for a ride around the city in his huge Cadillac.
"Listen," he said, as we were returning, "is it true that not only are you a missionary, but also the son of a missionary?"
"Yes," I said, "and my grandfather and two great-grandfathers were also missionaries." He gazed at me in awe.
"Then how does it happen you are not an imbecile?"
In Namkham we played baseball and went on picnics with the nurses. They went with us when we took a joy ride in the car. Tiny had them over to an occasional meal and tea party.
They would come and play Monopoly and Chinese Checkers at the house. We went through their hardships with them and they went through ours with us. We were with them when they were well and took care of them when they were sick. We figuratively spanked them when they were naughty---and made them like it.
The only way we could make financial ends meet was with our fees. These would have been enormous if the hospital had been located in a city, but Namkham is just a country town with only a few wealthy people, and they are both miserly and very, very nationalistic. That is, they would pay a hundred rupees to a Shan quack, call me only when that quack had given them up for lost, and pay me five rupees---or at the outside ten.
Mr. Read, an Australian friend of mine for whom I had the most astonishing admiration, came to visit me. He loved to ride my ponies, but I couldn't arrange to ride with him myself. One night, just as he was going to bed, an obstetrics call came in from the top of the six-thousand-foot mountain behind the hospital. We went together on our two bigger ponies, and a couple of nurses trailed us on their smaller ones. We reached the village just before dawn and had a very difficult forceps delivery. While I was scrubbing up afterward he asked me how much of a fee I expected? "Well," I said, "I don't expect any. We never charge for a labor case, for I have too soft a heart for a woman in labor. But if they pay anything, it will be one rupee." Nothing happened till we were ready to mount, when a woman came running out and put into my hand just that amount: one rupee-thirty cents. But with those tiny fees, tens of thousands of them, we kept out of debt. Chinese coolies paid us nothing. Rich Chinese paid us almost enough for themselves and for the Chinese coolies. Kachins made us tiny token payments, and the Shans averaged just about what it cost to treat them.
DURING OUR first five and a half years in Burma, Dr. Harper died. His church at Detroit, desiring to build a lasting memorial to him, gave us twenty thousand dollars to build a hundred-bed hospital. Tiny and I had the plans all ready. The plans called for an expenditure of forty thousand dollars. It was up to me to find the other twenty thousand in Burma. We located just enough money to make up the amount lost in exchange transferring the money from Detroit to Burma. The Mission Property Committee in Rangoon, however, was in those days quite imaginative, and they felt I could get all but one wing of the hospital with the funds at my disposal, providing I built it myself. To a man of my temperament, that was like a red rag to a bull.
We decided to make the hospital out of cobblestone, unlimited amounts being available in the river beds within two miles of the hospital site. I telegraphed to my father to buy us a ton-and-a-half truck in Rangoon, ship it loaded to Mandalay by steamer, where Tiny and I would pick it up. On our way down in the Chev, we heard disconcerting rumors that trucks were not allowed to use the Mandalay-Maymyo road; but the truck was on the steamer, and my father had thoroughly loaded it to the skies, so that we had to stop every few miles as we drove along and pick up a couple of chairs or a box that had been knocked off by the branches of the trees. When we got to the foot of the mountain, there, by the side of the road, was a sign stating that trucks with a load capacity of more than half a ton were forbidden to use the road. And here I was with a ton-and-a-half truck, and was it loaded! There was nothing for it but to do what any other good missionary would have done. I turned the truck off the side of the road into the jungle and waited till it was almost dark, and then I started up that hill as fast as I could go with my foot right on the floor of the car!
Halfway up the mountain a horn sounded behind me. A huge car wanted to get past. And to the radiator of that car was tied an English flag. The only man in Burma permitted to fly the Union Jack on his car is the governor of Burma, and there was the governor himself. Was my face red? It was so red it made the governor think I was one of those hard-drinking British Army sergeants driving an Army truck! At any rate the governor said nothing, and we got our truck out beyond Maymyo onto the dirt roads of the Northern Shan States. Those Shan States roads are made of red clay that becomes very slippery indeed when it rains. And of course it rained. It always rains when I have to travel. And how that truck could skid! Tiny was following behind me in the Chev, until she saw me turn end for end several times, and then she insisted on going first. If her husband was going to do those foolish things, she thought she could stand it better if she didn't have to look on. So she went first, I came along behind, and in the first twenty-four hours we covered twenty-five miles. But we got that truck to Namkham.
Then we began to haul stone. We hired a few coolies to gather the stone, and then after the hospital work was done the nurses would pile on board and we would go out, throw the stones on, and haul back several loads. I asked my Chinese carpenter if he could estimate how much stone we would need. He could. He took the plans and a pencil and in a few minutes said we would need so many tons of stone. Later I discovered that if we had hauled as much stone as that Chinese carpenter told me to haul, the hospital would have been solid throughout like the pyramids!
On furlough in America I had picked up an old broken theodolite that Tiny's father had thrown away years and years before. My father and I took the theodolite, surveyed the hospital site, which was on the top of a hundred-foot hill by the side of the Bhamo branch of the Burma Road, leveled it off, and dug the foundation pits. Now we were all ready to build, but I had not the slightest idea how to begin. In my medical course in Johns Hopkins they had not taught me how to mix dental cement, even, let alone lime and sand mortar. But there was a missionary named Weeks in Moulmein who had put up a lot of fine buildings. I telegraphed him inviting him to spend his summer vacation in Namkham. He accepted, but could spare only one week. On the afternoon of the day he arrived for his "vacation" we started putting in the foundations, and by the time he left, a week later, we had one corner of the hospital built up to the tops of the windows of the lower story. Now I understood how to fasten those rocks together. His vacation had been such a success that I invited other knowledgeful missionaries to spend their vacations in Namkham. What a summer that was! At our meals together we ate and laughed so loudly they could hear us at the hospital a couple of blocks away.
Hundreds of tons of building material had to be brought in from Lashio, a hundred and thirty miles away. Tiny and I used to do this job together.
We started from Namkham at dawn and covered a hundred and thirty miles into Lashio by three in the afternoon, threw on a load of stuff, and started right back. When I became so sleepy that I couldn't drive, Tiny took the wheel. Once, after midnight, she was driving. I was sound asleep in the back of the truck with a half dozen barrels of cement. Suddenly she stopped the truck, so suddenly that the cement barrels began tumbling all about me, and screamed, "There is a tiger in the middle of the road. Wake up and shoot him." It all fitted in so well with a lovely nightmare I was enjoying that it took me some time to wake up; by which time the tiger had disappeared.
Another day at noon, we stopped just before hitting a giant leopard warming himself in the middle of the road. The leopard got up lazily and slipped over the side of the road into some bushes. I reached for my .32 rifle, got up on the hood, jerked down the lever to throw a cartridge from the magazine into the chamber, waited for the leopard to reappear. He never turned up, which was good for me because someone had unloaded the gun and stolen all the cartridges!
Aside from three good Chinese carpenters for the woodwork and, later, a fine Indian chap to do the plastering, most of our work was done by Shan and Kachin coolies, and a great deal of it by voluntary free labor. We chose half a dozen of the most intelligent and taught them to be expert masons for cobblestone work. The roof was completed just as the rains were breaking. Then we put in the electricity and plumbing. Mr. Smith, professor of physics in Rangoon, put in my Pelton wheel-dynamo outfit, but I had to do the plumbing myself. I was determined to have modern plumbing even if I had no hospital. All the piping was ordered in Rangoon, cut to what I thought were the right lengths, with both ends threaded. As long as the pipe was correct in length, it was quite easy. But when it was too long, I had trouble. I could cut the pipe to the right length, but I could not afford a set of dies to cut the threads on the end of the new pipe, so I had to pull out my hack saw and make the threads. By dint of sawing threads and fastening things together, the plumbing was all in and everything worked splendidly: but before long the whole system was stopped up from top to bottom. You see, the patients would throw not only paper but gauze dressings, sticks and even stones into the toilets. So I had to take the plumbing apart, clean it, and put it together again.
Not having to pay out half our funds to contractors, we not only completed the entire building according to the plans, but had a much more firmly constructed building, since we had used tons and tons more cement than the specifications called for.
But we had no money left for beds. All I could do was saw up the lumber from the scaffolding and use it for beds. Termite-ridden, it furnished the most wonderful hide-outs. Passing through a ward one day I saw a nurse down on her knees with a crochet hook in her hand jabbing at one of the beds. I stood by and counted. She got fifteen out of each crack!
When we moved into the new hospital the nurses used the old wooden building for a home.
The new building filled up rapidly, until it was running to capacity. But we were not satisfied. We were not reaching the countless sick in the jungles who were too ill to travel. We felt we ought to have branch hospitals and dispensaries out in the wilds where we could place graduate nurses. The girls had had an overwhelming experience in the wards with the common diseases of the country so that they knew almost as much about them as I did myself, and, after all, it was those diseases they would be sent to treat. Anything unusual that they did not understand, they could send in to me. We opened three hospitals in our second period of service, one thirty miles west, one forty miles east, and one a hundred miles, as the crow flies, to the east of the Salween River. The girls were all graduate midwives as well as nurses, and the good they did was immeasurable. I had given no special obstetrical or surgical instruments to one of the girls as I felt she might not be too clever in their use. But one day she was called twenty miles away for an obstetrics case. When she arrived at the house the baby had been dead three days, wedged tight in the pelvis in the transverse position, its body decomposing very rapidly. The nurse asked for a scissors, and the family produced a rough Chinese bazaar product. With that scissors the nurse disarticulated the child's shoulder, removed the viscera, delivered the child, and the mother actually lived. Another of the nurses, faced with a similar transverse presentation but with the child still living, propped her obstetrics notebook up on the floor, scrubbed, made the husband pour chloroform, and delivered a live baby.
In the last year of our second term of service, an insignificant-appearing road was built for automobiles, running north from our Lashio-Namkham road to Chefang, in China, a total distance of about thirty miles. The Lashio-Namkham road was also continued over an enormous suspension bridge to Bhamo, the head of shipping on the Irrawaddy. These roads ran right through our hospital's sphere of influence. We hoped the road would continue north to Chefang and Mangshi, but didn't suppose it ever would.
Part Two: Burma Road
Table of Contents