
THOMAS W. EVANS, M.D., PRESIDENT OF THE AMERICAN INTERNATIONAL SANITARY COMMITTEE.
SIR;
 S the causes which brought us together
have now no existence, and as the work of the American ambulance
is nearly finished, and I am about to leave Paris, I deem it my
duty and also my privilege to lay before you in as concise a manner
as possible the surgical history of the ambulance, that through
you, the general, and medical and surgical public may become possessed
of all matters of moment which have occurred during my administration.
S the causes which brought us together
have now no existence, and as the work of the American ambulance
is nearly finished, and I am about to leave Paris, I deem it my
duty and also my privilege to lay before you in as concise a manner
as possible the surgical history of the ambulance, that through
you, the general, and medical and surgical public may become possessed
of all matters of moment which have occurred during my administration.
You may remember that my connection with the ambulance commenced on the 7th of September last. At that time all the tents were pitched in the position which they afterwards held; their location, surroundings, and the material of which they were manufactured, met with my hearty approval ; and when the floors, drains, and heating apparatus were added, I considered that nothing more, in a sanitary point of view, was to be done. Barracks were subsequently constructed, adding two large airy wards for the reception of wounded men, while other portions were set apart for the dispensary, surgeon's office, operating-room, post-mortem-room, and many other offices which did not come under my supervision.
In short, when complete, the hospital was nearly perfect, leaving little to be desired either as a flying ambulance or a permanent institution.
![]() FTER the extraction of all the
foreign matter possible--- including such fragments of bone only
as might have been detached from the periosteum---the wounded
regions were covered with several folds of cloth, in the form
of a compress, dipped in warm water. This was enveloped in some
impermeable material, such as oil-cloth, cotton, or silk. In some
instances, sheets of thin india-rubber, which is equally impermeable,
were used as a substitute ; though this objection has been urged,
that it is a good heat conductor, and hence becomes readily cold
on moderate exposure to the air. If this objection has any weight,
the difficulty can easily be obviated by covering the rubber with
any non-conducting material. The dressings were made daily---when
necessary, twice a day---care being taken that no part of the
dressing was used a second time, if not thoroughly washed and
purified.
FTER the extraction of all the
foreign matter possible--- including such fragments of bone only
as might have been detached from the periosteum---the wounded
regions were covered with several folds of cloth, in the form
of a compress, dipped in warm water. This was enveloped in some
impermeable material, such as oil-cloth, cotton, or silk. In some
instances, sheets of thin india-rubber, which is equally impermeable,
were used as a substitute ; though this objection has been urged,
that it is a good heat conductor, and hence becomes readily cold
on moderate exposure to the air. If this objection has any weight,
the difficulty can easily be obviated by covering the rubber with
any non-conducting material. The dressings were made daily---when
necessary, twice a day---care being taken that no part of the
dressing was used a second time, if not thoroughly washed and
purified.
The wounds were carefully washed, cleansed, or injected with dilute carbolic acid or the preparations of chlorine. Dilute alcohol was sometimes used. The first agent was also used in stronger solutions to deodorize the dressings.
The wounds when unhealthy, or not sufficiently active, were stimulated with nitric acid, of the strength of one hundred and twenty drops of strong acid to the quart of water. This solution was also applied to swollen and oedematous parts with seemingly good results. Sulphate of copper was also used---one to two drachms to the pint of water---the proportion depending upon the condition of the parts requiring stimulation.
Warm water applications, oil-cloth coverings, &c., either in the form above indicated or in the shape of linseed poultices, have been used in inflammatory action, or when pus was forming, with great comfort to the patients.
In flesh wounds, after full suppuration had been established, the parts were properly supported by compresses and bandages, to prevent the accumulation of pus or other matter.
To keep the dressings still further free from offensive odours, the parts were constantly surrounded with oakum, which acted simultaneously as a compress, disinfectant, absorbent, and deodorizer.
Opium, morphia, and chloral, were given in various forms to assuage pain and to produce quiet and sleep; valerianate of zinc to allay nervousness; chloroform and ether were used as anæsthetic; desiccated alum, perchloride of iron, and ergotine were applied to arrest hæmorrhage; iodine was locally used to reduce any thickening, as well as in certain abnormal conditions; soap and water, or molasses and water, were generally employed for injections; laxatives consisted mainly of rhubarb, seidlitz powders, purgative lemonade, citrate of magnesia, castor-oil, and black-draught.
In compound and comminuted fractures, to avoid the accumulation of pus and other matters in the tissues surrounding the wounded parts, india-rubber drainage tubes were introduced and retained until the parts had so far healed as to obviate the necessity of their further use. Through these tubes, warm water, dilute nitric acid, dilute carbolic acid, dilute alcohol, weak chlorinated waters, or any other deodorizers, purifiers, or stimulants, can be easily injected, as the case may require. These have the double effect of freeing the parts from decomposed tissues, blood, pus, or other discharges, and of washing to the surface any débris of devitalized bone or other foreign matter, the presence of which might be prejudicial to fragments of bone still covered by and adherent to the periosteum.
There is nothing so destructive to newly-forming or formed plastic matter, or to a periosteum, the circulation of which is enfeebled by violence done in crushing the bone and tearing its blood-vessels, nerves, &c., as the presence of large accumulations of putrid, offensive, and acrid discharges, imprisoning as they do sloughs and other foreign matter. If to this are added great shortening of the limb from spasmodic contraction of its muscles, and the compression and arrest of circulation at the seat of and surrounding the injury, frequently occasioned by the surgical appliances---those enveloping the entire limb, such as impermeable coverings of plaster of Paris, felt, pasteboard, &c., or any other surgical apparatus for restoring and maintaining even an approximation to the normal status of the fractured limb---we have, I apprehend, all the conditions necessary for delayed reparation of the injury, to say nothing of the almost constant bony necrosis which ensues, and which is a prolific cause of death.
In order that cleanliness might be properly effected and maintained, the clothing and bedding, when soiled, were immediately replaced by that which was clean and fresh.
The barracks and tents---in order to carry out as far as possible all hygienic measures---were from time to time emptied of their occupants, and thoroughly fumigated with chlorine gas, disengaged on an extensive scale, and somewhat in the following manner :---Several large vessels or dishes were placed at equal distances along the centre of the tent or barrack, as the case might be, containing equal quantities of peroxide of manganese and common salt moistened with water. The tent or barrack was then closed, and a sufficient quantity of strong commercial sulphuric acid was thrown simultaneously into the vessels. Immediately the ward was filled with thick vapours of chlorine gas.
After the chemical action had fully subsided, the board floors were taken up, the ground cleaned, swept, and covered with sulphate of iron, and the floor replaced.
The floors, when swept, were from time to time sprinkled with a mixture of sulphate of iron and sand, which was allowed to sift through the crevices to the ground ; occasionally a solution of permanganate of potash was used instead.
Ventilation was effected by a combination of means, but chiefly by a constant current of cold air passing over a heated surface, and thence along a trench under the floor of the tent, thus also keeping the ground and floor perfectly warm and dry.
From this source the air re-absorbed moisture, of which it had been deprived in its passage over the heated surface, and was then distributed to all parts of the tent, displacing the foul air.
GENERAL SURGICAL TREATMENT OF COMPOUND FRACTURES.--- As injuries of the long bones and their joints are frequent and often of great gravity, it is not surprising that differences of opinion should have existed among eminent surgeons as to the most feasible plan of treatment which would save the most lives and give useful limbs.
The treatment adopted at our ambulance was in the main such as I have laid down in a report of surgical experience in the treatment of compound fractures during the Peninsular Campaign of 1862, read before the Medical Society of the State of New York in February, 1863, and again substantially reiterated in February, 1864, in an article discussing the proper mode of treatment of "compound and comminuted gunshot fractures of the thigh, and the means for their transportation." In the article referred to the treatment is stated as follows :
"1st. In cases where the artery or arteries are destroyed, or so lacerated as to cut off circulation below the wound, and gangrene is the inevitable result.
"2nd. In cases where a limb is torn nearly or quite off, as by a solid shot or any other analogous missile, leaving an irregular or ragged stump.
"3rd. In cases of extensive injury to the soft parts alone, where gangrene would be likely to follow from the loss of the principal nerves or arteries.
"4th. In certain cases of compound and comminuted fracture of the knee and ankle-joints. The passage of small balls which do not shatter or open the joints do not necessitate amputation, and particularly is this true of the ankle-joint. Compound and comminuted fractures of the femur, or tibia, which extend into the knee-joint, require amputation."
"1st. Excision should be confined to the upper extremities--- the shoulder and elbow-(joint) being the principal parts upon which that operation should be practised.
"2nd. If the head of the humerus is shattered by a gunshot, excision is the only remedy. If the comminution extends to the shaft, the loose portions only which are deprived of periosteum need be removed, the residue should be left to granulate. If the glenoid cavity is crushed, its loose spiculæ can be removed or its injured portion gouged out.
"3rd. If the elbow-joint is crushed or comminuted by a ball, excision is the only remedy. 1f the injury is confined to the articulating end of the humerus, remove it, but do not disturb the ends of the radius or ulna; if the injury be confined to the articulating ends of the radius, or radius and ulna, remove both, but not the humeral articulation.
"If the articulating ends of the humerus, radius and ulna are crushed, remove them all. What is meant in the books by partial excision is the removal of a portion of the joint, such as a part of the humeral articulation, or the articulating end of the radius or ulna only.
"The removal of the entire half of the joint results in a new articulation, and not in anchylosis, as is often the case in partial excision. If the comminution extends to the shaft of the humerus, or radius, or ulna, remove its loose spiculæ, and leave the rest to nature.
"4th. In comminuted compound fractures of the carpal end of the radius, or radius and ulna, excision of the articulating ends affords the most reasonable prospect of success. Leaving it to nature is far preferable to amputation. Never amputate for this injury.
"5th. Compound gunshot injuries of the carpus or metacarpus seldom, if ever, require either excision or amputation. Remove the loose bones, and treat as a simple wound.
"6th. In compound gunshot injuries of the phalanges, excision can be practised only with varied success, owing to the size of the bullet and the smallness of the member. The rule is to save as much as possible. Injuries to these parts sustained by buckshot or pistol balls do not, as a rule, require amputation. On the contrary, most of them can be saved.
"7th. In compound and comminuted injuries of the humeral shaft, excision or amputation should never be performed. The loose spiculæ should be removed, and the case treated as an ordinary compound fracture. If, however, the comminution extends to the articulation, it (the articulation end) should be excised with the loose spiculæ, while the fragments of the shaft which still retain their periosteum should not be disturbed.
"8th. The same rule applies to the shaft of either or both bones of the forearm. In all cases avoid constriction by bandaging.
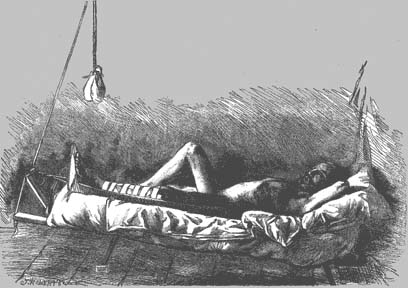
"9th. Cases of compound, or compound and comminuted gunshot fractures of a portion of the femur, not involving the knee-joint, ought to be treated as hereinafter detailed, viz., by simple extension and counter-extension---making the stretcher the splint.(1) (See Fig. 50.)
"10th. Cases of compound and comminuted gunshot fractures of the tibia, or tibia and fibula, not involving the knee or ankle-joint, should be treated as above stated for the femur.
"11th. Simple gunshot injuries of the ankle-joint do not necessitate amputation, while compound and comminuted fracture of this joint, and particularly when the arteries are much injured, may require amputation; though with proper support, water-dressings, irrigation, free incisions, &c., a great majority of these cases will recover without operative interference.
"The rule applicable to gunshot wounds of the hand is also applicable to those of the foot; and I can safely say that there is scarcely a bullet wound of the foot which requires amputation. I have seen the whole scaphoid bone carried away, and still a good recovery take place. So the destruction of the astragalus may occur, and still recovery go on favourably. See the case of Garibaldi, in whose ankle-joint a ball remained for some months without unfavourable results.
"12th. In compound and comminuted gunshot injuries of the tarsal and metatarsal bones the same rule of action should be adopted as in like injuries of the hand, with the exception, that a slight deformity is not of such importance in the former as in the latter.
"13th. No excision or amputation should be performed in the second or inflammatory stage.(2) If the operation cannot be performed before this stage sets in, we ought to defer operation until the truly second, or suppurative stage, appears."
In military surgery, the necessities of war compel the surgeon to conform his treatment to the exigences of the occasion as much as possible. This is particularly true in cases of gunshot fracture of the leg and thigh. It is said that the transportation of soldiers after amputation of either of these members is less troublesome than before, whatsoever form of support is given to the limb. Insomuch, therefore, as active warfare requires the constant movement of armies, it behoves us, as surgeons, to improvise means whereby fractures can be placed under treatment while on the field, or as soon after as possible, before the soft parts are irreparably injured by being torn and cut by the sharp ends of the broken bone in the process of transportation. The treatment should be continued without any violent change which would endanger life or prejudice the results.
If this can be done without deranging or increasing the embarrassment attendant upon the transportation of wounded men; if means can be adopted by which compound fractures can be safely transported---no additional burden being imposed upon the ambulance trains; if, at the same time, the appliances necessary for the treatment of such fractures and those requisite for transportation can be so simplified as not to increase the labour of the surgeon, we have, I apprehend, the solution of the question at issue. For, in my opinion, the whole subject is summed up in the word transportation.
It is now proven beyond a doubt, that when wounds of this character are placed under treatment, before too much additional injury is done in the process of transportation, if proper surgical treatment is adopted, a larger number will recover than from amputations, and that, too, with sound and useful limbs.
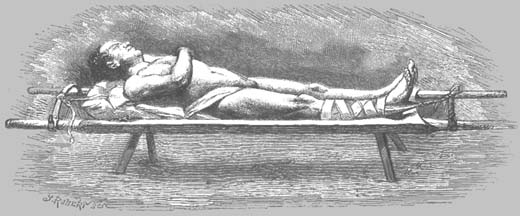
| FIG. 50.---Stretcher arranged for the transportation and treatment of a case of compound fracture of the leg or thigh. During treatment the foot of the stretcher can be elevated to make the weight of the body the counter-extending force, and thus temporarily release the groin from the pressure of the perineal belt. |
By what plan, then, can all these ends be accomplished? The answer is simple, and the treatment is equally so. There are always supposed to be a sufficient number of stretchers on the field, and if not, a few additional ones can be supplied. Experience shows that the number of gunshot fractures of the thigh and leg not involving the knee-joint is very small in comparison with the great number of flesh wounds of the lower extremities. During the War of the Rebellion in the United States, there were, up to a certain period, thirty thousand gunshot injuries of the lower extremities, of which less than five thousand involved the shaft and knee-joint.(3)
Suppose that each fracture of the leg or thigh were represented by a stretcher, this would not materially add to the difficulty of transportation.
To the ordinary American or French stretcher I would add two semi-circular spurs of iron, each having at its end an iron ring, so made as to fit the handle of the stretcher, and provided with a thumb-screw. One spur is slipped on the handle of the stretcher by means of the ring, and is fastened at the proper angle by the thumb-screw. From this spur, extension can be made by attaching a piece of cord to the sole of the foot. The loop is made by extending adhesive plaister from the knee down one side of the limb and around the foot. The other spur is placed on the other end of the stretcher. From this, counterextension can be made by the perineal belt. In order that there may be no misconception of the plan proposed for the transportation and treatment of compound fractures, I append a sketch (Fig. 50) of a person under treatment on such a stretcher.
This stretcher, therefore, becomes the bed, the vehicle for transportation, and the splint for the treatment of the fracture.
The wounded man, after being properly dressed on the stretcher---extension and counter-extension having been made---need not of necessity be transported until the limb is consolidated. If thus dressed, the patient can be carried any distance, stopping as often and as long as circumstances may require.
On this stretcher the wounded man can be borne with perfect safety to the limb, by hand, in cars, in boats, or in ambulance waggons built to receive the litter, or even in common freight railway waggons, provided they are so arranged that the weight of the body may rest upon the extreme ends of the stretcher. In this way the elasticity of the wood from which the stretcher is constructed is utilized, and the bruises or injuries avoided which might ensue from the shocks and jolts produced by the roughness of the road over which the carriage passes. No number of consecutive stoppages, either for hours or days, could in any way interfere with the process of restoration, provided the man be as well cared for as at first, and not removed from the stretcher.
In the treatment of fractures by this method, all necessary sanitary measures can be employed. Without the least possible delay, trouble, or change in the surgical appliances, or derangement of the injured limb, the patient with his bed can be removed from whatever may be offensive or insalubrious to any place where the most approved sanitary and hygienic measures can be adopted ; while any soiling from discharges of blood, pus, urinary, or fæcal matter, can be washed from the canvas covering of the stretcher on which the man lies, without doing violence to the injured limb.
If at any time it becomes necessary to use the stretcher as a means of temporary treatment during the transportation of the fracture, the perineal belt can be dispensed with and counterextension be continued by raising the foot of the stretcher.(4) This may seem paradoxical; but when the principle is examined it becomes undeniable. It is upon this plan that I have for many years treated fractures of the thigh, whether simple or compound, and at whatsoever point the fracture may have been located.
In 1849 an article was published by me in the "Transactions of the Medical Society of the State of New York," describing the manner and mode of treating fractures of the thigh by extension and counter-extension. The principles were the same as those indicated above, with the exception that in making the extension, when the bed was used, the head and foot of the bed were made use of in place of the semi-circular spurs described as applicable to the stretcher.
Again, about 1859, I published another article in the "Transactions" of the same Society, recommending the treatment of all fractures by simple extension. I have followed this plan of treatment with unvarying success, with such modifications as the circumstances required. The result has been that in simple fractures of the thigh the longitudinal and lateral distortion were so slight as to be with difficulty discovered on inspection, or even by measurement.
When wounds or excoriations existed which prevented the use of the perineal belt, I adopted the expedient of raising the foot of the bed, thus converting it into an inclined plane, against which the weight of the body would rest and act as a counter-extending force, obviating the necessity of a perineal belt.
Long after the publication of the articles referred to, and after this treatment of fractures had proved successful, Dr. Gurdon Buck, of New York, conceived the idea of carrying out this principle by using weights and pulleys as the extending force, and of effecting counter-extension by means of a small elastic india-rubber perineal belt. He also encircled the thigh with short longitudinal strips of split deal, which were sustained by thin elastic india-rubber bands. This he called Gurdon Buck's method of treating fractures---a very delicate kind of professional plagiarism, since, unless the principles involved in this practice were new to him, he was hardly disposed to give credit to him to whom credit was due. I had the satisfaction, however, of seeing many persons treated in the New York Hospital by "Buck's method," and found that the results did not compare with those obtained by permanent extension; and that while no lateral distortion existed, the shortening from overlapping was too great to be consistent with a simple fracture. I have no doubt that this condition was due partly to the smallness and great elasticity of the perineal belt, which would allow the weights to rest on the floor, or the body to slip to the foot of the bed; partly to the impossibility of adjusting weights to various degrees of muscular strength and physical power; and partly to the interference of nurses and others, who, at the solicitation of the patient, would remove the weights temporarily, thereby retarding the efforts of nature towards reparation.
It was generally conceded that the principle involved in the treatment of fractures of the thigh, proposed by Dr. Gurdon Buck, was the same as that which I had advocated and practised ---namely, extension and counter-extension----and which many surgeons at a meeting of the Medical Society of the State of New York declared could never be successful.
Dr. Buck, therefore, in deference to the general opinion, added a fanciful improvement for coaptation (the strips of split deal), which was of no more use towards effecting the result desired than would have been so much tissue paper encircling the thigh; it served only to satisfy the patient and his friends.
I must, however, do him the justice to say that in the treatment of gunshot fractures of the thigh, with loss of bony substance, the weight and pulley serve an excellent purpose for extension; but the weight should be so adjusted as to obviate the possibility of its finding support on the floor, and thereby becoming useless. Instead, however, of using the perineal belt for the counter-extension in permanent treatment, we would advise the use of the body only, as in a case described further on.
![]() ROM the beginning of the siege
to the 30th of November, 1870, above sixty wounded men were treated
in the ambulance.(5) Of
these but two died; and the immediate cause of their death was
tetanus. Four of the above number were amputated through the thigh
for wounds of the knee-joint; two compound fractures---one through
the neck and one through the shaft of the femur---were successfully
treated by conservation, and are now well, walking with crutches,(6) and possessed of good limbs;
one compound fracture of the tibia, just below the knee, recovered,
but afterwards received an injury in another part from which he
died;(7) two gunshot fractures
of the wrist and two of the ankle-joint recovered with useful
limbs; two comminuted fractures of the scapula, a number of gunshot
fractures of the bones of the forearm, hands, feet, and fibula,
one resection of the shoulder-joint---for compound fracture of
the head of the humerus---in a soldier suffering from large pleuritic
effusion, one wound through the chest---ball passing through the
right lung, entering the third rib anteriorly, and passing out
posteriorly under the scapula---besides several other serious
cases, not particularly interesting in a surgical point of view,
were successfully treated.
ROM the beginning of the siege
to the 30th of November, 1870, above sixty wounded men were treated
in the ambulance.(5) Of
these but two died; and the immediate cause of their death was
tetanus. Four of the above number were amputated through the thigh
for wounds of the knee-joint; two compound fractures---one through
the neck and one through the shaft of the femur---were successfully
treated by conservation, and are now well, walking with crutches,(6) and possessed of good limbs;
one compound fracture of the tibia, just below the knee, recovered,
but afterwards received an injury in another part from which he
died;(7) two gunshot fractures
of the wrist and two of the ankle-joint recovered with useful
limbs; two comminuted fractures of the scapula, a number of gunshot
fractures of the bones of the forearm, hands, feet, and fibula,
one resection of the shoulder-joint---for compound fracture of
the head of the humerus---in a soldier suffering from large pleuritic
effusion, one wound through the chest---ball passing through the
right lung, entering the third rib anteriorly, and passing out
posteriorly under the scapula---besides several other serious
cases, not particularly interesting in a surgical point of view,
were successfully treated.
We now come to a period extending from the 30th of November, 1870, to the end of the siege, in which food and fuel insufficient quantity or of proper quality were not to be had, so that all the wounded whom we received, much exhausted from exposure and want of food and fuel, were in a condition unfavourable for surgical treatment. Many were suffering from the usual camp diseases, such as diarrhoea, dysentery of a typhoid character, and chills, and fever. Others had been lately discharged from hospitals, where they had been under treatment for the prevalent diseases bronchitis, pneumonia, and pleurisy, and sent to field duty, and were therefore still very feeble. Indigestion was the rule when food was taken; while some were unable to eat even when suitable food was offered. Subsequently to this period the mortality was increased, owing to the causes above enumerated, and to the mortal nature of the wounds. For example, from seventeen shell wounds received from Drancy in one day, eight died in a short time from their wounds. Still later during the siege several died from acute pulmonary disease superinduced by deficiency of fuel. Some of the deaths, as will be seen by reference to the history of the fatal cases, occurred immediately on or a few hours after arrival, while others whose wounds were equally mortal shared the same fate at a later period. It is therefore scarcely necessary for me to add that the greatly increased mortality after the 1st of December was due to causes over which surgery had no control.
It is proper to state in this connection that all our wounded were brought to us directly from the battle-field, or had received temporary surgical attention only, prior to their transportation to the ambulance.
The gentlemen volunteer aids, whose duty it was to go to the field with the carriages to pick up the wounded, made it a point to seek and take in the most severely wounded, and particularly those having fractures, as it was believed that this class of wounded, especially, would suffer less under tents than in houses. In thus selecting the severely wounded, many would of necessity be brought in who were so gravely injured as to be amenable only to palliative treatment. An additional reason for our having obtained so large a number of this class of' wounded, was that these gentlemen were generally in advance of all others.
These facts explain why among the 247 surgical cases treated at the ambulance, there were 126 compound fractures.(8) Notwithstanding this great number of fractures and the causes previously enumerated, only 47, or a little over 19 per cent., have died of their wounds. The following table gives the number of fractures classified according to the region involved.
| Hip-joint |
4 |
| Thigh |
3 |
| Knee |
7 |
| Leg |
7 |
| Ankle |
10 |
| Head of humerus |
9 |
| Scapula and clavicle |
12 |
| Arm |
6 |
| Elbow |
4 |
| Forearm |
9 |
| Wrist |
4 |
| Hand |
11 |
| Head |
10 |
| Face |
7 |
| Chest |
10 |
| Back |
9 |
| Pelvis |
4 |
|
|
126 |
Notwithstanding the large number of fractures, conservative surgery was so extensively practised, that of the 126, only nine seemed to require amputations of the long bones.
The results of these cases, as a whole, in spite of the adverse conditions previously mentioned, will compare favourably with those of a similar class in other wars, though the latter class may have been treated under much more auspicious circumstances.
Again, if we take into consideration the sixty cases received prior to the 30th of November, and treated before the depressing effects of the siege were felt, no results, either in public or private practice, could have been more satisfactory; for, with the exception of the accidental loss of two from tetanus, there were no deaths.
Only three gunshot fractures of the shaft or neck of the thigh have been received in the ambulance suitable for conservative treatment; all the others have involved the knee-joint. The above-mentioned were treated by extension and counter-extension ; two, (Cases 3 and 4,) without the pulley; and one, Case 134, with the pulley and weight alone. Case 3 was fractured in the neck of the femur, Case 4 in the middle, and Case 134 at the juncture of the lower and middle thirds.
All recovered with comparatively little shortening and no lateral distortion, as may be seen by reference to their histories, which contain much matter of interest.
CASE 3.---Corporal Jules Melchior, 2nd Company, 3rd Battalion, 35th Regiment of the Line, was wounded September 30th, 1870. A ball entered on the inner side of the left thigh, about one inch below the angle formed by the scrotum and the thigh, fractured the neck of the femur, passed upwards, outwards, and backwards, and had its exit through the gluteal muscles. On arrival he was weak from great loss of blood. The limb, which was greatly swollen, distorted, and shortened, was placed in a wire gutter padded with oakum, and covered with hot-water applications and oil-silk. It was then sufficiently extended and fastened to the foot of the bed. This was effected by placing strips of adhesive plaster on one side of the limb from the knee, around the sole of the foot, and up to the knee on the opposite side. These strips were held in place by bandaging the limb as in Case 134 (see Fig. 54). A cord was then passed through the loop of plaster on the sole of the foot, and fastened firmly to the foot of the bed or stretcher. Extension and counter-extension were made by converting the bed into an inclined plane, by raising the foot of the bed. Against this the body rested, and thus effected the extension, sufficient to keep the limb and body in a normal line without impeding the circulation or confining the parts. The patient suffered no pain after the dressings, and continued to improve, and also to eat and sleep well. His only medicine was generous living. During the first twenty days several small fragments were discharged from the posterior wound; at the end of this time the anterior wound had closed, and the limb was found to have shortened about three-fourths of an inch. The limb continued to improve until November 10th, forty-one days after the injury, when union seemed very strong. November 20th, fifty-one days after the injury, there was great periosteal and interstitial thickening of the whole shaft of the femur---so much so, as to give it the appearance of having been fractured, with distortion. This was treated and reduced by the tincture of iodine, hot-water applications and oil-silk. At this time union seemed quite firm. Gradual improvement up to January 20th, one hundred and twelve days after the injury, when the patient was able to rise. Three days after, he began to walk with crutches, and continued to do so for six days, with no inconvenience on bearing the entire weight of his body on the injured limb. However, upon careful examination it was found that additional shortening had resulted. It was then thought best to remand the patient to bed and apply extension for several days. The periosteal thickening greatly diminished---the limb had been otherwise in excellent condition, and the patient was in enjoyment of perfect health. He was discharged entirely well on the 1st of March, 1871. On this day photographs of his limb were taken, woodcuts from which are here appended (Figs. 51, 52).
 FIG. 51.---Appearance (front view) of the limb of Corporal Jules Melchior at the time of his discharge from the ambulance and five months after the injury. |
 FIG. 52.---Appearance (lateral view) of the limb of Corporal Jules Melchior at the time of his discharge from the ambulance and five months after the injury. |
CASE 4.---Private Jules Hardy, 3rd Company, 2nd Battalion, 35th Regiment of the Line, was received September 30th, 1870. His injury was a fracture of the middle third of the right femur, the central portion of' the shaft being shattered through a length of fully five inches. The ball entered posteriorly about the middle of the shaft, was split into two fragments by the fractured bone, making two exits anteriorly. The patient on arrival was much weakened from loss of blood. The limb was shortened about five inches, and was distended to its utmost capacity by an effusion of blood within the fascia lata. The limb was placed in a gutter padded with oakum, and covered with hot-water applications and oil-silk, and extended and counter-extended, as in Case No. 3, before described. During the whole course of the treatment quinine and iron were given. October 20th, twenty days after the injury, a fragment of bone, constituting the entire thickness of the shaft, was removed. October 25th, a second piece, similar to the former one, was removed during suppuration. The periosteal sides of both fragments were entirely smooth, showing that they had just been detached from the periosteum, while the other presented a worm-eaten appearance. The bone was found to be consolidated about November 10th. November 17th, pretty firm union; no lateral distortion; fully two inches shortening; no thickening except the fragmentary consolidation. December 2nd, one of the anterior wounds closed. December 15th, the posterior wound closed, but re-opened December 26th, at which time, upon careful examination, pieces of dead bone were found firmly attached. January 15th, a small abscess formed and was opened near the seat of the fracture. January 20th, the limb was found to be firmly united, with about two and a-half inches shortening. At this time extension was taken off, and the whole limb and foot were bandaged to sustain proper circulation. January 25th, gastric irritation set in with severe vomiting; for three days the patient was unable to retain anything on his stomach except champagne and ice. After that attack his health returned, and he continued well up to the 5th of February, when there was more gastric irritation, but of a milder form. Stimulants and milk were then administered with success. February 10th, he was able to sit up for a few hours a day. February 14th, he was able to bear, without inconvenience, much weight on the injured limb. February 20th, his face and body were somewhat œdematous; his urine was examined and found loaded with albumen. Appropriate remedies were given to combat the disease. There was steady progress up to March 4th, the patient continuing to walk with crutches. still albuminous, but limb well and strong. On the 7th there was very considerable oedema of the legs, giving to the wounded limb the appearance of deformity. A photograph was then taken of the patient, a woodcut from which is here appended (Fig. 53). On the following day the oedema had disappeared, though the urine was still heavily loaded with albumen, and he left for his home in the country, well, with the exception of the diseased action of the kidneys.(9)
| FIG. 53.---Appearance of the limb of Private Jules Hardy twenty-one weeks after his injury. |
CASE 134.---Private Zépherin Vautier, 2nd Company, 1st Battalion, 7th Zouaves, was received November 30th, 1870; his injuries were a fracture of the left femur, and a flesh wound of the right thigh. A ball had entered through the rectus femoris, about six inches above the knee- joint, and passing through the femur, had been divided into three pieces, one making its exit near the gluteal muscle ; another was extracted on the posterior surface of the limb, nearly opposite the point of entrance; a third remained just under the skin, two inches above the exit of the last-named portion of ball. The limb was shortened about three inches, and enormously swollen from infiltration of blood in the fascia. The patient suffered little pain. His general condition, to all appearances, was good. The fractured limb was placed in a wire-gutter or splint padded with oakum, dressed, and the extension made as in Case 3, except that the pulley and weight were added, as shown in the accompanying sketch (Fig. 54). The limb was examined from time to time, and found doing well. January 4th, it was entirely re-dressed; it was then found that all the wounds were healed except at one point, where a splinter of the ball was being thrown out by suppuration. The general condition of the patient was always good. One of the remarkable features in this case was, that all the wounds, save the one in the gluteal region---from this there was a small discharge of pus and fragments of bone---healed without any appreciable amount of suppuration. At this time there was about one-and-a-quarter inches shortening of the limb, some union, considerable bony enlargement, but no lateral distortion. The limb continued to improve, and by the middle of January the man was up. The evidences of fracture were these:---1. That the limb would bend freely at the point of fracture, notwithstanding the enormous swelling from the effusion of blood. 2. That there were fragments of bone imbedded in the pieces of ball. 3. That fragments of bone were discharged from the wound in the gluteal region. 4. That there was, and is, over an inch of shortening. 5. That the bone at the seat of the fracture was and is much thickened. 6. That there was great bony crepitation.
| FIG. 54 shows Case 134 under treatment for compound fracture at the juncture of the lower and middle thirds of the left thigh; the adjustment of the weight and pulley is also shown |
March 6th, this patient was discharged well, the fracture firmly consolidated, although at that date he walked with crutches. His appearance is shown in the accompanying sketches from photographs taken at the time (Figs. 55, 56).
 FIG. 55.---Appearance (front view) of Private Zépherin Vautier thirteen weeks after his injury---a gunshot fracture of the left thigh. |
 FIG. 56.---Appearance (lateral view) of Private Zépherin Vautier thirteen weeks after his injury. |
To show further what has been done in this direction, I call attention to the report of the Surgeon-General of the United States ("Circular No. 6," S. G. O., 1865), which is replete with interest, because of the vast number of gunshot fractures of the thigh and the knee-joint recorded.
|
or of Gunshot Wounds of the Knee-Joint, out of 3,106 Cases that have been entered on the Records. |
||||||||||||||
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Gunshot Fractures of Femur, implicating Hip-Joint |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Gunshot Fractures of upper third of Femur |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Gunshot Fractures of middle third of Femur |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Gunshot Fractures of lower third of Femur . |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Gunshot Wounds of the Knee-Joint, with or without Fracture |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| R= Recovered D= Died U=Undetermined MRDC= Mortality Rate of determined cases |
||||||||||||||
"In examining the above table in detail, it is seen that the results are ascertained in 822 of the 1,263 cases treated by amputation, or 65 per cent.; in 64 of the 82 cases treated by excision, or 78 per cent.; and in 1,117 of the 1,761 cases treated by conservative measures, or 63 per cent." It further shows, that of the 1,117 terminated cases treated by conservation, 71.26 per cent. died; while of the 822 terminated cases of amputation, 63.26 per cent. died; leaving 8 per cent. in favour of amputation. It must not, however, be forgotten that there were 644 of the former undetermined, while there were only 441 of the latter under treatment. I doubt not that the results of the unfinished cases will change the balance-sheet in favour of conservative surgery. The report further states, in way of explanation, "that the amputations include most of the bad cases, and those in which preservation of the limb was attempted and abandoned." I do not fully understand what the "Circular" means by "bad cases," unless it is that they are all wounds which destroy the knee-joint, or so fracture the bone and lacerate the soft parts as to require amputation. In such cases, there is nothing to be done but to amputate. The writer of the above either forgets or fails to state that in these cases amputation is generally performed upon the field and without much delay; they are therefore mainly good cases for amputation.
The good results obtained under adverse circumstances in the treatment of the class of gunshot fractures, above referred to, and summed up in "Circular No. 6," convince me that the difference in the percentage of recoveries between amputations and conservations was due to the excessive inflammation occasioned by insufficient protection of the fractured limb during long and tedious transportations over bad roads, or no roads at all, and by the delays and breaking of communication by steamboats and railway. Besides, the necessities of war, in some instances, compel leaving the wounded on the field of battle for days together. This was the case in the Seven Days' Battle of the Peninsular campaign, in the Battle of the Wilderness, and in many other instances. My opinion upon this subject is strengthened by reference to a report of the comparative results obtained in the Crimean War between amputation and conservative treatment. Professor Legouest there shows, that of 337 wounded, having compound fractures of the thigh, and treated without amputation, 117 recovered fit for service.
The fractures are thus divided as regards the seat of the injury and the results :---
|
|
|
|
|
|
| Of the neck of the femur |
|
|
|
|
| In the trochanters |
|
|
|
|
| In upper third |
|
|
|
|
| In the middle third |
|
|
|
|
| In the lower third |
|
|
|
|
| Without indication of seat of fracture |
|
|
|
|
|
|
|
|
|
|
In this connection he shows that, of 1,666 amputations performed only 123, or 7.40 percent., survived; while of the 337 cases treated conservatively, 117, or 35 per cent., survived. In other words, the number of amputations of the thigh recovered, compared with that of the recoveries by conservation, shows that "there four times as many recoveries" from the latter treatment as from the former:---" That in fractures of the lower part of the thigh, the number of recoveries from non-amputation exceeds that from amputation. And, finally, that in fractures located above the middle of the thigh, there are twenty-four non-amputated cases surviving and not one amputation."
He then proceeds:---
"To give the relative results obtained from amputation and conservation in different parts of the shaft. For the upper third of the femur, as 31.50 is to 6; for the middle third of the femur, as 34.75 is to 6; for the lower third of the femur, as 42 is to 10. The ratio of these tables is as 35 is to 740; that is to say, there is very nearly five times more chance of recovery from a gunshot fracture of the thigh without amputation than there is with amputation."
In his concluding remarks on the conservation of the thigh he states:---
"That the practice of amputating the thigh, in consequence of a gunshot fracture of the femur, which maintained its supremacy so long without contestation, seems destined to-day to give place to that of conservation of the limb."
Should it be argued that there must be other causes assigned for the great disparity in the comparative number of deaths from amputation and conservation in the Crimean War, I should answer that the general statement is, that of the 1,664 amputations of the thigh performed in the French army, 1,541, or 92.60 per cent., died. But a more careful analysis shows that of the 1,541 deaths
| 781, or 46.93 per cent., | died in the Crimea; |
| 278 " 16.70 | at Constantinople; |
| 482 ," 29.00 | on their way to France, |
| 1,541 |
Thus it appears that only 46.93 per cent. died before removal, while 45.67 per cent., or about one-half, died en route, or in hospitals far removed. Also, that amputations cannot be removed, or even roughly handled at a very early period, without a fearful mortality resulting therefrom. I have shown conclusively, in a former part of this report, that compound fractures of the thigh can be removed any distance without more encumbrance to ambulance trains than cases of recent amputations, and with greater safety, if we consider the results obtained in the French army as a criterion.
There have been seven amputations of the thigh performed at the American ambulance.
Of these, five were wounded through the knee-joint.
The sixth was wounded just below the knee-joint. From this wound he had recovered, when he received an injury above the knee, which necessitated amputation at the upper third. From the effects of this second injury he died. The case is full of interest, and is given under the head of "History of each case which terminated fatally."---Case 8.
The seventh was wounded just below the knee-joint. An india-rubber drainage tube was passed through the track of the ball. Two days afterwards, however, it was found necessary to amputate through the knee joint, owing to great effusion in the tissues below the joint, which destroyed their vitality. The patient did well up to the twenty-fifth day, and was considered out of danger, when, on account of a deficiency in fuel, he suffered and died. (See Case 222.)
One of the above five cases, after he was considered out of danger, died of tetanus. (See Case 7.)
A second on arrival was unable to retain food. He reported that for several days preceding his wound he had suffered from vomiting and other symptoms of gastric irritability. He was wounded through the knee-joint, and the leg was completely infiltrated with blood and serum. Vitality had ceased, and amputation was performed without delay. But the patient failed to retain anything on his stomach, and though he lost little or no blood, either during the amputation or afterwards, he continued to sink, and died two days after the operation.
The histories of the three remaining cases are as follows.
CASE 5.---Private Alfred Doucet, 5th Company, 3rd Battalion, 35th Regiment of the Line, was received September 30th, 1870. His injury was a fracture of the articulating portion of the tibio-femoral end of the femur; the ball had entered posteriorly, and lodged between the condyles, crushing that portion of the femur into several pieces and opening the joint. Amputation was performed, by an anterior flap, at the lower portion of the middle third of the thigh. The limb was dressed with sutures, oakum, compresses and bandages, and covered with oil-silk. Subsequently, adhesive plaster was applied in addition to the above, to keep the edges of the wound in place. October 26th, twenty-seven days after the injury, the patient was able to rise and sit in his chair. Thirty-two days after the injury he was able to walk with crutches. Fifty-five days after the operation the wound was entirely healed. The limb has never since given any trouble, and the patient has been in good health. March 1st, the patient was discharged. At this date his photograph was taken, a woodcut from which is given in Fig. 57 (No. 2).
 |
|
| FIG. 57 shows the appearance of the limb of Alfred Doucet at the time of his discharge (No. 2), as also the appearance of the shoulder of Clement Daumont, March 1st, 1871 (No. 1) |
CASE 9.---Private Jean Buzier, 5th Company, 81st Regiment of the Line, was received September 30th, 1870. A ball had entered just above the joint to the left of the middle of the patella, and passed on, as far as could be discovered, externally to, and not involving the joint; it was removed from the posterior aspect of the limb about the middle of the gastrocnemius muscle. On arrival, the patient was suffering severely from loss of blood and violent spasms in the leg. These spasms, due somewhat to the exertion of walking some distance after the receipt of the injury, were prevented by splints applied to the limb, so as to obviate any motion. The limb was then covered with hot applications and oil-silk. Opiates were given in moderate quantities to alleviate the pain. Soon after the receipt of the injury, severe inflammatory action ensued. Large abscesses formed below and above the joint. About the 26th of October, twenty-six days after the injury, the joint was found to be diseased, and discharging large quantities of pus and dead tissue through the openings of the abscesses. From that time up to November 1st large and repeated doses of opium were required to keep the patient easy. The condition of the joint showed that the cartilages were severely inflamed. After a consultation on the 1st of November, thirty-one days after admission, it was decided to amputate. Amputation was performed by a long anterior flap. The joint was found very extensively diseased ; the cartilages and several portions of the articulating ends of the joint destroyed, the ball having chipped off a portion of. the articulating end of the tibia in its passage downwards. After amputation, gradual improvement followed, the wound healing kindly---much of it by first intention. On the eighth day after amputation an undue disposition of the muscles to retract was counteracted by the weight and pulley, applied by means of adhesive plaster around the stump. At the end of thirteen days the patient was able to rise. On the twenty-sixth day after the operation he was able to walk with crutches, the wound being healed, except a space of one and a-half inches, the site of an old abscess. The patient continued to do well up to January 15th, when he injured the stump by a fall. An abscess formed in the neighbourhood of the bone. February 14th, a small piece of carious bone was discharged from the end of the shaft. Notwithstanding this the patient was in perfect health. March 8th, a photograph was taken, which is here reproduced (Fig. 58, No. 2).
 |
|
| FIG. 58 shows the appearance of the limb of Jean Buzier (No. 2) at the time of his discharge; as also the appearance of the limb of Edmond Vernatier at the time of his discharge (Fig. 1). |
CASE 23.---Private Edmond Vernatier, 1st Company, 1st Battalion, 38th Regiment of Mobiles of the Seine and Marne, was received from Bourget, October 21st, 1870. A ball had passed laterally through the knee-joint, breaking the condyles of the femur. The patient was in good. health on arrival. Amputation was performed on the 22nd of October, between the middle and lower thirds of the femur, by a long anterior flap. The flaps were brought together with sutures, the wound dressed with lint, covered with oil-silk cloth and enveloped in oakum. On the twelfth day the wound was nearly healed, and mostly by first intention. On this day he had stiffness of the jaw, constriction of the muscles about the throat, and all the symptoms of approaching tetanus. The free use of cigarettes, containing each four grains of opium, controlled these symptoms for a time. At their reappearance the same treatment was followed. They lasted during three days. On the sixteenth day the ligatures came away. On the twenty-first day the patient was able to sit up. Twenty-eight days after the operation he was able to walk with crutches. He continued to improve, and was discharged to the convalescent ward within thirty days after the operation. January 20th, he was entirely well, and could go anywhere on crutches.
March 8th, 1871, Vernatier was discharged perfectly well, and his photograph taken, which is here reproduced (Fig. 58, No. 1).
In this connection it seems proper to call attention to the comparative results obtained in our ambulance between amputation and conservation in gunshot fractures of the femur.
The percentage of deaths in amputations compared with the results of conservations was as follows: seven amputations of the thigh were followed by four deaths and three recoveries, or 42.86 per cent. Three gunshot fractures of the thigh treated by conservation were followed by three recoveries, or 100 per cent.
A reference to the history of the four deaths after amputations of the thigh will show, however, that in no case was the amputation the immediate cause of the death, and that, moreover, none of these cases could have been treated conservatively.
There was one resection of the knee-joint for compound fracture, which proved fatal. (See case 116, under the head of "History of each case which terminated fatally.")