
THE AUTHORITIES IN BERBERA, the port of British Somaliland across the Gulf from Aden, were taken by surprise. A garbled message had led them to expect ten Quaker women missionaries, and the prospect of ten Quaker women had caused alarm and consternation. They turned out instead to be six men in Red Cross uniform wanting transport to Addis Ababa. It was the first week of August 1942, and the men were the first contingent of forty members of the F.A.U. who were on their way to Ethiopia.
The party of forty had left England in five groups. With the first were Richey Mounsey, the Commandant, and Michael Vaizey, the senior Medical Officer, who were to make advance arrangements. But the first to leave were not the first to arrive. No sooner had they left Liverpool than their boat broke down. It returned for repairs, set off again in three weeks time, broke down a second time and returned to Gourock. Abandoned by its convoy, ramshackling along or drifting aimlessly for hours with no power in the engines, it broke down thirty-four times between Gourock and Capetown, where, to put a fitting close to its adventures, a vital part blew up with a shattering explosion and a rain of metal on the deck. And that was the end of the boat for many months to come. The other groups had less adventurous journeys, and early in November 1942 all forty, converging from different directions, had reached Addis Ababa.
The central plateau of Ethiopia, on which Addis Ababa stands, itself eight thousand feet high, rises to the north in a riotous array of vast mountain ranges broken up by deep valleys and gorges, while to the south and east it merges into tropical forests, into the hill country of Kenya and into the arid deserts of Somaliland.
One Unit party entered from the north. Leaving the boat at Massaua, the port of Eritrea on the Red Sea, it moved inland to the capital, Asmara, the end of the northern route to Addis.
Here it was held up for a month because the road was declared unsafe ; there had been an outbreak of activity by shifta, the bands of brigands who infested the highways and were rendered doubly dangerous by the vast stores of Italian arms that had fallen into their hands. They were one only of the many products of unsettlement and unemployment caused by years of war. At last, when the party did leave, the journey to Addis took eight days. They passed along the metalled Italian road, through the upland villages of Eritrea, down sweeping escarpments where the road clung in precarious hairpin bends to the sides of the hills, then across the frontier to find themselves in Ethiopia. Thence the road took them south across the mountains, through Amba Alagi, Dessié and Debra Sina, over the crest of the Mussolini Pass, tour de force of Italian engineering, and on to Debra Birhan, ten thousand feet above sea level ; finally along the open pastoral country of the central plateau down into Addis Ababa itself.
The other four parties came in from Berhera, joining at Diredaua the Djibouti-Addis Ababa railway, the only railway in the country. The approach to Addis from the east was less impressive. From Berbera they journeyed by lorry through barren, sandy country, along a rough road to Jijiga, then inland over undulating hills strewn with boulders or covered with scrub. The road wound its way through the hill country up to Harar and on to Diredaua, and there they joined the train. It was the route along which the first of the armies eighteen months before had fought its way into the capital.
They found that Addis Ababa bore little resemblance to the European's conception of a capital city. Beautifully situated on an open plain and surrounded by high hills, it had a few streets which suggest a capital, a few large buildings, of which some were pre-Italian, while others were built or half-built during the occupation; many edifices, including a large opera house, still stood gaunt and empty behind a network of scaffolding, their building rudely brought to an end by the war. Otherwise the city resembled an enormous village, with miles of winding country lanes, with here and there Italian villas interspersed with corrugated iron shacks and the tukuls---huts of wattle and daub and thatch---in which the native Ethiopians live. Always the streets were thronged with people, ranging in colour from the pale chocolate of the tall and proud Amhara, dressed in white shirt and cloak, or shamma, and in tight cotton jodhpurs, to the jet black of the lowest of the menial workers, the despised Shankalla. An occasional touch of incongruity would be provided by the addition to the native garb of Italian uniforms and trappings, boots and battered trilbies or, topees. There was some Italian traffic, cars and lorries in various stages of disrepair, but for the most part vehicles were drawn by small horses, and Jehu-driven pony-traps served everywhere as taxis. On all sides there was a profusion of lofty grey-green eucalyptus trees and of the brilliant yellow mascal flower. For they had arrived at the end of the rains. Soon the ground would be caked and parched, but now it was green and carpeted with flowers and the climate was that of a pleasantly cool June day in England. For Addis, though nearer the Equator than Berbera or Massaua, avoids by its height their sticky, stifling heat.
Before the Italian invasion turned the eyes of the world upon it, Ethiopia was a land mysterious and remote, visited by few travellers, the romantic country of the south, reputed home of the Queen of Sheba and of Prester John. Little was known about it or its people. Estimates of its population in 1939 placed it at about ten million, of whom 130,000 were Italians settled there in the preceding three years. Under King Menelik, at the turn of the century, the Amhara, whose original home was in the hills south of Lake Tana, had conquered the surrounding tribes---the Galla to the south of Addis Ababa; still further south the Wollamo and Sidamo; the Somali to the east, and the tribes of Kafa to the south-west on the borders of the Sudan. To the north were the Tigrae, to the northeast the wild Danakil of the desert. Amharic became the official language, and the animist or Mohammedan faiths of some of the conquered tribes were assimilated, though by no means completely, to the Coptic Christianity of the Amhara.
The Italians constructed new buildings, they brought into the country good transport, they developed communications with well-engineered roads, they introduced some industrial plant and began mining operations. But against such material benefits were to be set the destructive and disintegrating effects of conquest and occupation. There had been wholesale executions of the better educated and patriotic Ethiopians. The towns had acquired a veneer of European development, but often of the worst and most depressing type.
When the Emperor rode into his capital on 5th May, 1942, it was to face a monumental task. Behind the glow of liberation were the inevitable disorders which in every country followed in its wake. Widespread unemployment and destitution, with their concomitants of violence and brigandage, were added to the centuries-old problems of primitive ignorance, illiteracy, superstition and disease. The central Government's authority in the more remote provinces was never strong, and there was no clear system of taxation to produce an adequate revenue.
A certain amount of the material development could indeed be salvaged, but if the country was to be built up on the Western pattern which the new Government had set before itself, there was need for assistance from outside. Against the proud independence of the Amhara, and their resentment of outside interference in the one African country besides Liberia that was autonomous, had to be balanced the plain fact that, when the Italians had done their worst, there were not enough Ethiopians to carry on the Government and social services of the country in the way in which the Emperor wished.
IT WAS IN APRIL 1941, while the war in East Africa was still in progress, that the Unit had first raised with the Foreign Office the possibility of sending an ambulance convoy to Ethiopia. The matter was referred to the War Office, and in July the Unit was informed that if a convoy were sent it would be needed mainly for civilian clinic work to assist the British Army doctors in the larger towns and the provincial areas. Negotiations went ahead, and in September 1941 a party of forty was assembled, particular preference being given to men who had spent the longest periods of training in British hospitals. They came together at Livingstone College, Leytonstone, which before the war was used as a missionary training college. There they were instructed in tropical medicine by Dr. Jays, the Principal, and in the elements of Amharic by Emanuel Abrahams, who was at the time attached to the Ethiopian Legation in London and later became a close friend of the Unit in Ethiopia itself.
Shipping had been arranged for the end of October. And then the delays began. Negotiations had started for an Anglo-Ethiopian settlement which was to transfer the control of the country from the armies that had reconquered it to the Emperor himself. It became clear that the War Office would no longer be concerned, and the Foreign Office was not anxious to push arrangements until the agreement had been concluded. Any assistance sent would now have to be at the request of the Ethiopians themselves. So the section was broken up for Unit work in England or for further training. Time was well spent in London at the Moorfields Eye Hospital and in venereal disease clinics or other departments of the London Hospital, Guy's, St. Thomas's, the Middlesex, the Royal Northern, and University College Hospital. The Unit always found a ready response from the larger hospitals to any request for the training of its men.
At long last, after months of waiting, the agreement was signed at the end of January 1942. The British Army was to be withdrawn except from certain reserved areas ; only a small Military Mission would remain behind to train the Ethiopian Army. It was now quite clear that the Unit's work would be different from what had originally been envisaged. There would be fewer Army doctors, and consequently the Unit would have to act more independently and bear greater responsibility. By good fortune two doctors had become available---Michael Vaizey, a member of the Unit Council who left the staff of the London Hospital for the purpose, and Anthony Husband. On 7th April a cable arrived from the Emperor himself inviting the section and undertaking to provide its maintenance, and six weeks later the first party made its abortive attempt to get away.
It is important to understand what job a wartime body like the Unit was going to do. The Italians had built up a medical service in the country; there were hospitals in Addis Ababa and in the larger provincial towns, where ambitious medical buildings had been constructed, while there were clinics in the smaller centres of population. It is said that during the occupation there were a thousand Italian doctors in the country, their main concern being presumably the health of the Italian settlers. But every hospital had its wing for native Ethiopians, if for no other reason than that the health of the settlers would be endangered by disease among the native population. Then suddenly, with the Italian defeat, the whole fabric collapsed.
A few Italian doctors, some twenty-five in all, were left behind, mainly in Addis Ababa and one or two of the larger provincial towns. There was only one Ethiopian doctor in existence, and he was not practising. Apart from twelve British Military Mission doctors, mainly of Palestinian nationality, whose main concern was the Ethiopian Army, and three British Red Cross doctors in charge of a hospital in Addis Ababa, that was all. The Military Mission doctors were attached to Ethiopian battalions, and could devote only their spare time to civilian work. A handful of foreign sisters and nurses completed the picture except for a number of Ethiopian dressers, mainly Italian-trained, some good, some indifferent, and many very bad.
It was obvious that slowly the Ethiopian Government would have to build up its own medical administration by attracting qualified doctors on a considerable scale from overseas. The problem was a permanent one, though largely complicated by the war, and palliative action would only put off the day when something had to be done. A temporary voluntary organization was no sure basis for the "Ministry of Health" of a country many times the size of Britain, and the Unit went out in the full realization that its function was a limited one, to fill a gap, for a year in the first place, with the possibility of extension while a more adequate and permanent service was developed. When it arrived it found that it was in fact to become well over half the official medical services of the whole country. In Syria the Spears Clinics had never been more than a supplement to the Government services; in Ethiopia the Unit had all the advantages and disadvantages of being incorporated into the official scheme, officially financed and, as far as the job was concerned, officially controlled.
 |
 |
The section on arrival reported at a large Italian building, once intended for a hospital, in the main thoroughfare of Addis Ababa, Churchill (late Mussolini) Street ; here the Ministry of the Interior was installed. A floor of the building was occupied by the Medical Directorate, which was in fact the country's Ministry of Health. Its total staff consisted of George Maclean, the Director of Medical Services, who was responsible to the Ministry of the Interior, and was the one European in the country in an executive position (all other European servants of the Government were advisers to the Department concerned); Colonel Aitken, his assistant; an Egyptian with his Czech wife, who between them acted as secretary, book-keeper and interpreter ; an Italian driver and salaries clerk ; and Greek and Egyptian interpreters.
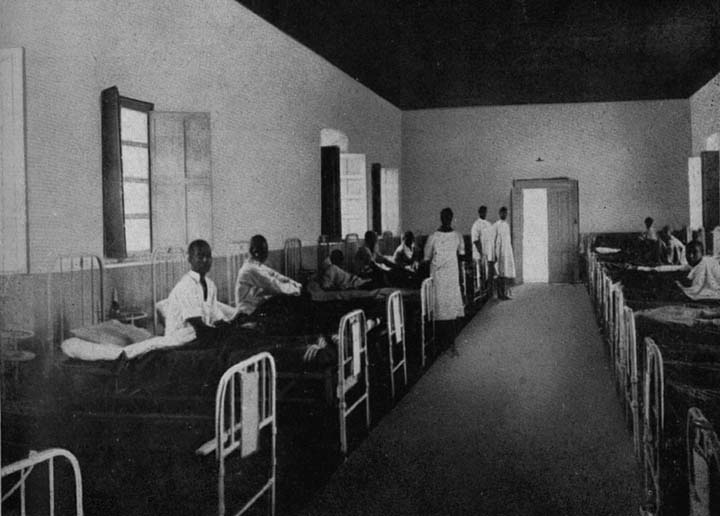
The Directorate's responsibilities were wide but not clearly defined. In Addis Ababa three of the five hospitals were Government ones. The largest was the Menelik Hospital, intended mainly for Ethiopian Army patients; it was largely financed by the Directorate but run by the Military Mission with several of its own doctors assisted by Ethiopian dressers paid out of the Army budget. It had about three hundred military and civilian patients. Near the market-place, providing a free service for pauper patients, were the shoddy wooden buildings of the Hammanuel Hospital, at the time in charge of three Italian doctors. When members first visited it they were sickened by the stench and over-crowding patients lay on the floor in filthy rags or else two to a bed, covered with a tattered blanket. Cross-infection on a large scale was inevitable. The Directorate's third responsibility was the Italian Hospital, later to be called the Ras Desta, which catered for well-to-do Ethiopians and Italians, its fees providing for the Government some sorely needed revenue. There were two independent establishments---the Haile Selassie Hospital, a large and well constructed stone building, the private property of the Emperor, which was run by Dr. Last of the British Red Cross, with the help of two assistant doctors who left soon after the Unit's arrival, and of three British sisters, and the Filwoha Maternity Hospital conducted by a Seventh Day Adventist Mission.
Four clinics completed the medical service in the capital, of which three came under the Directorate.
Outside Addis Ababa the services depended almost entirely on the Military Mission doctors, and they were an uncertain prop for a civilian system, since if their battalion were moved they were moved too. Elsewhere a few scattered clinics struggled along with Ethiopian dressers who were often short of the most elementary drugs and equipment. Many had carried on from Italian times; the Medical Directorate had no full record of the dressers who were supposed to be in its employment, and for many months to come men of whom no one had heard would turn up in Addis from the provinces asking for their wages. As for the Italian doctors left behind, few would face the provinces. In the capital and in the larger towns the standard of life was less primitive, and they could supplement their income by private practice. In any case there was a prevalent fear that the provinces might not be very safe.
The Medical Directorate thus had its cup full of the problems of a country which was trying to stagger to its feet after eight years of war and foreign domination. Of its many and varied difficulties the two most persistent throughout the Unit's stay in Ethiopia were the total inadequacy of its financial resources and the constant uncertainty and bickering over the control of its budget and its policy. When the Unit arrived £150,000 had been budgeted for the Directorate for a whole year, but during the first six months only a quarter of this sum was received. The wages of dressers remained unpaid or fell into arrears, and were in any case hopelessly inadequate. A junior clerk in a Government office was often paid twice as much as a skilled dresser. One provincial hospital reported "the pay of a Head Dresser was 52s. a month. The average wage for the staff was 44s. and the average family consisted of a wife and two children. On even a frugal diet this family required 50s. for teff (the standard grain) alone ; this did not take into account other essentials. Those fortunate enough to own land made up the deficit by doing a little farming in addition to their hospital work; others were forced to draw on capital left over from Italian times, or else were more or less starved and ragged." So the work became one long struggle to carry on with a totally inadequate budget; and what budget had been provisionally agreed was constantly being cut in favour of other departments the work of which was apparently more important than the health services. To try to minimize the difficulties of the Government would be the height of folly ; but it was the Medical Directorate that always seemed cast for the rôle of Cinderella.
With little appreciation at the time of this background, the Unit on its arrival discussed how best it could fit in. It was normally Unit policy to work together as a group, and to assume responsibility for a particular piece of work. But now it was a case of spreading inadequate numbers to make the most effective impact on a vast need. So it was arranged that there should be no separate Unit office, but that Richey Mounsey, the Commandant, with Jack Frazer, his Deputy, should work on the staff of the Medical Directorate and be responsible mainly for its accounts and transport, while Harold Waller came in as secretary to Colonel Maclean. Unit workers in the field were similarly responsible to the Directorate; the control and disposition of personnel was retained by the Unit officers but the work came under the Directorate. This policy was furthered when, in January 1943, Colonel Aitken resigned and Michael Vaizey became Deputy Director, a position which he occupied until near the end of 1944.
The Unit's final disposition was made with five obvious needs in mind. In the larger hospitals, in order that Military Mission doctors might devote what time they had to the clinical side, it was essential that all administrative detail should be taken off their shoulders, and so some men were assigned to hospitals as secretary-quartermasters, to do the work which would be done by the secretary or lay superintendent of a British hospital. Secondly, there were, in the comparatively well populated area around Addis Ababa---in the province of Shoa---several clinics in which members could work on their own so long as they were visited and supervised by a medical officer coming out from Addis Ababa. Thirdly, there was crying need for more Ethiopian dressers. The main difficulty in making any advance with Ethiopian students was their lack of general education. Many of them had been taught, and well-taught, to carry out certain routine and mechanical processes they could give "murfis" or injections (in Ethiopia, as in Syria, regarded as the panacea), and apply dressings, but, while there were exceptions, the majority were constantly handicapped by their ignorance of elementary arithmetic and anatomy, and of any language in which technical terms could be expressed. A scheme was therefore started for attaching a number of young probationers to the Menelik Hospital to receive practical nursing training and at the same time be given courses on a broader basis by two Unit members. Fourthly, as in Syria, clinical medicine inevitably led on to public health. There was little point in curing maladies in hospitals or clinics if the sources of infection were still left lying around for all to see in the garbage tossed into the streets, in the lack of any sanitation, in the mosquito breeding grounds or the fly-ridden slaughter-houses. A mobile hygiene unit was formed to work in one or two towns in improving the sanitary arrangements and to answer emergency calls to deal with epidemics. And lastly, just as clinical medicine leads on to public health, so it in turn leads on to the basic need for education. Some Unit members found themselves engaged full-time on educational work; others, when established in their hospitals and clinics, stole an hour or two day to teach in the local school, because they became increasingly convinced that this was ultimately the only answer to Ethiopia's need.
It soon became obvious that the Unit had not enough doctors at its disposal, and early in 1943, with the Emperor's agreement, a request was sent home for more. Five were recruited ; when they arrived towards the end of the year they greatly strengthened what contribution the Unit was able to make, and incidentally brought with them £2,500 worth of special drugs that were badly needed.
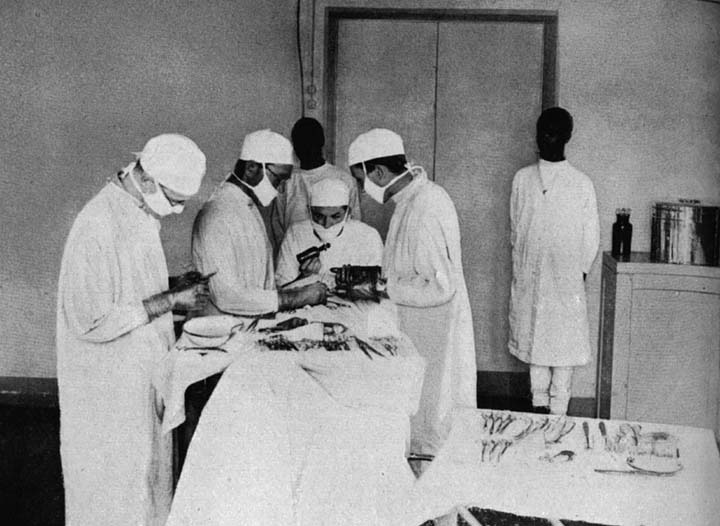
THE UNIT HAD LEARNT in theory in London what diseases it would be called upon to face. At the Menelik Hospital on their arrival members had some short practical training and experience. As common as in Syria were eye diseases of all kinds---trachoma, conjunctivitis, corneal ulcer, trichiasis and other conditions, many of which were caused or complicated by the widely prevalent venereal diseases. Malaria was rife in the lowlands towards the south, more rare on the central plateau or the northern mountains, except when it was brought up from the swampy tropical valleys. The register of one hospital run by the Unit for over two years lists in order of frequency, next to eye diseases and the very common wounds caused by accidents and fights with Italian fire-arms, the following: syphilis, skin diseases, tropical ulcers, digestive diseases, dysentery and rheumatism. Leprosy and typhus were to be found, the latter particularly at certain seasons. There were outbreaks of smallpox and relapsing fever and a high incidence of tapeworm caused by the habit of eating raw meat at festivals. Other more exotic diseases mean nothing to a layman but made Ethiopia, clinically speaking, a doctor's paradise.
Their patients had often been dependent on quacks little better than the medicine-man of Central Africa. They had a pathetic faith in charms and in branding with hot irons which made it almost impossible to detect a rash, already difficult to recognize on a dark skin. Often a patient would come into the clinic with half his calf eaten away by a foul and sloughing ulcer, over which he had tied a bit of string bearing a small silver cross or amulet made by melting down the Maria Teresa dollars which were one of the many currencies in the country.
In Addis it was possible to get to work straight away; as for the provinces, the first problem was to get there. There was only the one railway, that ran down through Hadama and Diredaua to Djibouti. Of road transport the Medical Directorate had only one three-ton Ford and one 15-cwt. pick-up, both only capable of facing a journey to the provinces if they carried their own mechanic and as many spare wheels as possible, anything from five to a dozen. An expedition into the country was always an adventure, even with reliable vehicles. Often on aged Italian vehicles it would mean climbing steep escarpments in reverse because that was the lowest gear, waiting a day or two at the roadside for the next vehicle to come along to give a tow, spending hours taking engines to pieces and putting them together again, until at last time ceased to matter. The main roads had been metalled by the Italians, but they were falling into disrepair, and a metalled road with large pot-holes is much worse than a mud road without. The element of danger from shifta soon raised the question of the armed guards who regularly accompanied convoys. The Unit's policy was to refuse guards if Unit members alone were involved, but if convoys were going out with other personnel and Medical Directorate stores, they could but accompany them.
The distance from Addis Ababa to Gondar as the crow flies is less than that from London to Glasgow, but by road it is nearly a thousand miles. For the first Unit party the journey took two days short of a month, such was the terrain and the quality of the transport provided. So also the original journey to the far south will give some indication of the difficulties of travel, in a country in which nature's barriers were as nothing compared with man's insistence on a wiriquet, the all-powerful bit of paper with a rubber stamp which was one of the worst habits learnt by the Ethiopians from European officialdom. Hugh Brown with an Italian doctor and an Italian laboratory technician left Addis Ababa on 26th October. When they reached the block-post just outside the town the Ethiopian official in charge declared that their pass did not mention the arms which the guards were carrying. One cannot bluff one's way past an Ethiopian official without a wiriquet. The party had to return to get the Public Security Department to alter the pass. This was eventually done but when they reached a point two hundred miles south of Addis a day a day and a half later they were again stopped. This time the official pointed out that their pass did not mention their two vehicles, so they had to stay two nights near the town until the matter was straightened out. Eventually they were allowed to proceed. But now nature took a hand. When they reached Ghidabo, they found the road bridge across the river broken down by the rains. They were loth to go back; it had been difficult to get so far as the road was in bad condition, and their trucks were heavily loaded; the tyres too had been punctured at exasperatingly frequent intervals.
So the next day the smaller vehicle was sent on by a circuitous route along an evil-looking track, where track existed, through several fords to arrive eventually at the other side of the Ghidabo bridge. The load from the big lorry was transferred with much labour and wetness to the other bank and loaded on to the small vehicle, which made several journeys to their destination.
Such problems of transport were for a time to prove one of the main stumbling blocks to the smooth course of the work. Some months after the arrival of the Unit Jack Geen was placed in charge of the Medical Directorate transport, a garage was opened, second-hand lorries were bought, and a system of proper maintenance and servicing instituted, with Ethiopians working under Italian mechanics. Spare parts and engines were obtained and breakdowns became less frequent. It became possible to have four or five lorries on the road at the same time. It was better than what had been, but it was still hardly sufficient to cater for the medical services of a whole country.
THE UNIT''S WORK can be divided geographically into three main areas: Addis Ababa itself ; the Shoa clinics in Ethiopia's "Home Counties"; and the more remote provincial hospitals which had infrequent contact with the capital.
In Addis Ababa itself, where the section lived in two Italian villas in Casa Incis, in the lower part of the town, the main centre of work was the Hammanuel Hospital. Robert Cook had been installed soon after the Unit's arrival, to work as secretary-quartermaster with an Italian doctor. The state in which he found the Hospital has already been described. The patients were paupers from the market-place, or orphan children who ran wild in the streets and made a precarious living by petty thieving, one of the most intractable legacies of the war. Water was brought by the municipal Fire Brigade, while the sewage, with no regular cesspit, found its way into a neighbouring churchyard.
Robert Cook remained in the Hospital throughout his period of service in Ethiopia and gradually built up a competent staff; he cleaned up the Hospital, made inventories, regularized the issue of food from the kitchen, and arranged for a piped water supply and septic tank, the effluent of which was used to irrigate a vegetable garden. Blankets and sheets were bought, but never in as large quantities as were required.
In due course the Unit took over the Hospital completely. First Dr. Michael Vaizey, and after him Drs. Tony Husband, Ken Llewellin and Pat Griffin came in. Three medical officers together in one hospital were a luxury which no other place enjoyed, but they were needed. Between January 1944 and March 1945 there were nearly six thousand admissions, over one thousand of them being infectious cases. Sometimes the Hospital was full to overflowing, as it was during a typhus epidemic at the end of the 1943 rains.
The one black spot in the Hospital which the Unit, for lack of personnel, was able to do little to improve was the ward of the mental patients; they were chained to their beds because there was no other way of coping with them, and the Unit was never able to change the system.
Other hospitals were helped from time to time. For a few months a secretary was provided for the Ras Desta ; Unit members worked with Dr. Last at the Haile Selassie, and at the Menelik Colin Prior and Glyn Johns ran the courses already mentioned for young probationer dressers.
The out-patients department for the Hammanuel Hospital was provided in the market place by the Tekla Haimanot clinic, which was under the care first of Tom Barnsley and then, when Tom became Second-in-Command of the section on Jack Frazer being moved to the Middle East, of Leslie Clarke.
A short distance away on a hillside outside the town was the Addis Ababa Leprosy Camp. Before the Italian occupation it had been run by an American Mission with a doctor and trained nurses. The Italians had extended it and numbers grew. The last Italian doctor to pay spasmodic visits to it had resigned and, in addition to the Tekla Haimanot clinic, Tom Barnsley assumed responsibility for the camp. When he arrived there was one resident Ethiopian dresser and an administrator ; they were both keen but had no special knowledge or training. In thirty tukuls of stone, overcrowded and dirty, were two hundred and forty lepers, young men and women in whom the disease showed itself only in the slight discoloration of the skin, chronic cases in which the flesh was being progressively eaten away. They complained of the complete inadequacy of food and of the bitter cold at night. What mattresses and blankets they had were in foul condition. The only water available was carried by mule from the bottom of the hill.
Lack of funds made it difficult to do much more than palliate their pitiful condition, but a certain amount was achieved. An attempt was made to produce more substantial food, and the small hospital attached to the camp was re-opened for regular treatment by one or other of the Unit doctors resident in Addis.
One job could certainly be done. There were many children in the camp who had not contracted the disease, their ages ranging from a few months upwards. Many were looking after their sick parents.
It was decided to segregate all children under twelve and, if possible, to remove immediately from their leper parents all babies born in the camp. The second step was not a success, but the segregation of the children was possible. On the edge of the camp was a large stone house which had once been occupied by the doctor. Here a children's home was started, with an admirable Ethiopian matron to look after them. Arrangements were made for extra milk and food, land being cultivated for vegetables; toys were procured, a handloom for making cloth and materials for mat-making. There were regular medical inspections, and after a time, if the children showed no sign of the disease, they could be declared clear. Finance was a constant anxiety, but in spite of it there was encouraging progress; the Unit contributed out of its own funds and, when it finally left, was able to arrange for the continuance of the work.
THE SIX MAIN CLINICS in Shoa were all within a radius of eighty miles from Addis Ababa. Indeed, to call them clinics is doing them an injustice ; in most cases they had a number of beds for in-patients who were serious enough to be detained but did not justify a journey into Addis. To start each centre one of the doctors went down with one or two men to take over old buildings which in some cases had fallen into complete disrepair, to clean them up, make good the damage, and fit them out as clinics and dispensaries. Then one of the Unit men would be left to it.
Regarding Addis Ababa as the centre, let us follow the six clockwise. Due north of Addis Ababa the small town of Fiché stands on the edge of a vast and wonderful gorge, south of the mass of mountains which hide the sources of the Blue Nile.
On the slope of a hill a short distance away from the huddle of native tukuls and Italian shacks, is a stone house that looks not unlike a Cotswold farmhouse; the back of it looks down a sheer two thousand feet to a tributary of the Blue Nile, with vast crags rising stark and forbidding beyond. It was by the window from this side that a leopard once entered the bedroom by mistake. Shading the front door stands a large and gloomy tree, sacred to the villagers who often bring their small offerings and place them under it. It is whispered with awe that an Italian major who once occupied the house dared to cut down a branch that was darkening his windows, and that same day he died. There lived Ken Tipper with two young Ethiopian boys. Apart from a Greek who ran the local store, he was the only white man in Fiché.
Between the house and the clinic at the other end of the village stood the Coptic Church, with crowds of beggars, diseased and halt and blind, clustering around the door, as they do everywhere in Ethiopia, holding up their hands with the cry, "Abeit ! Abeit!" At the far end of the village, past the prison and the school, the clinic itself consisted of a small hut for one or two in-patients, a larger hut for out-patients and minor operations. Out-patients numbered thirty-five to forty-five a day. The local authorities had proved co-operative and encouraged visits to the school and the prison to give treatment. Leaving the routine clinic work to the Arab, Tigrae and Amhara dressers on his staff, Ken spent part of his day teaching English and arithmetic and hygiene in the school.
Where the hand of the clock points to one, there stands another mountain town even higher than Fiché, the wild and barren Debra Birhan, ten thousand feet above sea level. Here in a land of roaring waterfalls and eagles, though only nine degrees from the Equator, three or four thick blankets are needed at night. When the advance party had gone, Jock Reid was left behind to carry on, no doubt inured by his native Orkneys to the wild and raw life of Debra Birhan ; he was joined for a time by his fellow countryman, Jim Milne.
In the clinic accommodation was established for twenty-five in-patients ; out-patients came in a steady stream. Patients came regularly from a radius of forty miles; some from Karakori, a hundred miles away. Malaria was uncommon, except when patients were brought up from the hot plains beyond Debra Sina, but the climate meant that there was always a great deal of pneumonia and influenza and some typhus. Later two sub-clinics were started, with Ethiopian dressers in charge, at Shano and Debra Sina.
Continuing round the clock, the hand at a minute or two past three o'clock points to the town of Hadama, near the malarious valley of the Awash. In a large Italian mushroom growth, native tukuls and ugly modern shacks were jumbled together in confusion around a vast open market-place, from the baked earth of which the wind swept the dust up in clouds, with the result that Hadama was notorious for its eye diseases. Bartie Knight was left here by the Unit, the only European in the town except for an Italian family in a nearby mill. A curious gentleman of many races, but basically Caucasian, had patched up a generator to produce for the town a somewhat shaky supply of electricity.
The hospital at Hadama was found in a set of barn-like buildings. What had been two wards were occupied, one by men of the Territorial Army and the other by the dressers. In two tiny rooms the Ethiopian dressers saw their patients, and in two more rooms, completely empty of any furniture, a few sick patients lay in their own rags on a broken concrete floor..
The Unit's efforts produced a ward with nine beds, a small operating theatre, a store, and a latrine dug as far away from the hospital as possible.
Hadama was a market town of some importance, and soon the out-patients department was seeing up to 150 patients a day ; a feature of the clinic was the separate room that was set aside for eye treatment.
More accommodation was required, and at last, in December 1943, after much negotiation, the Emperor's local residence was loaned for the purpose. In a large squarish bungalow, with a vegetable garden attached, it was possible to set aside wards for twenty beds, and separate rooms for stores, laboratory, office, out-patients department, and eye clinic. Attendance in outpatients grew to an average of over 200 daily, and reached a record on one occasion of 304. New clinics were started in Mojo and Hawash with a dresser in charge.
On the way to Hadama by road one passes through Bishoftu twenty-five miles only from Addis Ababa, a village close to a large and lovely lake that nestles among the hills ; unfortunately mosquitoes also find it lovely. Here the Unit had been given a cordial reception. The small clinic on the roadside was taken over, and John Grimwade, with the constant backing of the Mayor, found it possible to induct the townspeople into elementary rules of hygiene. Latrines of a deep pit type were dug in the centre of the town with corrugated iron over them; on market days they became fashionable, until sometimes there would be a queue awaiting entry. In due course, hoping that the Mayor's interest and the skill of the senior dresser, with regular inspections from Addis, would ensure the continuance of the work, the Unit withdrew.
But unfortunately, such is the Ethiopian lack of trained manpower, the Mayor was soon moved to a Public Health job in Addis Ababa and, without his guidance and inspiration, the work went rapidly downhill.
At eight the hand of the clock points to Wollisso on the road out to Jimma and the south-west. It was the last of the Shoa clinics to be started and the first to be closed. Its main trouble was accommodation. A petrol kiosk on the roadside was not the best place in which to hold a clinic, and it soon became overcrowded as the number of patients crept up into the region of 150 a day. In vain were attempts made to secure better quarters for the clinic and for Denis Roberts who was in charge, and when deadlock was reached in June 1943, the only solution was withdrawal.
Finally, eighty miles from Addis Ababa due west lies Ambo, built around hot sulphur springs which well up between the rocks. Here too accommodation caused trouble and the Governor would do little to help because there was some flaw in the wiriquet with which the Unit had originally arrived. At first Tony Husband and Norman Pollitt (who was later followed by Paul Wakelin) lived in a tent and then in the clinic building itself---a practice which the Unit always discouraged because of the danger of infection. Eventually a shop in the main street was made available and converted into a clinic room.
In all the Shoa clinics the development was the same-clinical treatment, public health and as much responsibility as the local authorities would allow to be assumed for the health of the prison and school. Indeed, this was the pattern followed in all the provincial areas in which the Unit worked.
The success of a busy out-patients department depended largely on the quality of the Ethiopian dressers who carried out the treatments specified. In time, with patience and regular instruction, most members gathered round them satisfactory teams. Some, like Bekele, the head dresser in Hadama, were outstanding.
"He was a remarkable young man. He became a very skilful and expert eye dresser, ran the dispensary, organized the feeding arrangement for in-patients, gave anæsthetics, did minor operations with abscesses and suturings, arranged rotas of duty, mixed drugs, did most of the more difficult dressings, accompanied me on tours of inspections to other towns and clinics or did them by himself. After he had been with me about a year, his Grade III as a dresser seemed rather absurd. He went to the Menelik Hospital for a fortnight's test and a regrading. In forty-eight hours he returned with Grade I."
And there was the head dresser at Debra Birhan. When the Unit first arrived the hospital was found to be in better shape than most, largely because of the efforts of Hakim Gizao, a local dignitary of considerable age, who had once been a student in Russia. He had wisdom and an aristocratic charm of manner. To occupy his retirement he had appointed himself senior dresser in the clinic, and after the looting which followed the Italian collapse he made a house-to-house search for the plunder-drugs and equipment and pieces of hospital furniture. Such was his standing that no one dared say him nay.
Everywhere some responsibility was taken for the local school, and most headmasters were only too anxious to be helped. That at Bishoftu, a training school for the Ministry of Agriculture, was found in a shocking state. Indeed, a reported epidemic there was the reason for the Unit first visiting the town. There was a great deal of disease and overcrowding, and the only bedding consisted of two filthy cotton sheets for each child. The quarters swarmed with flies, most effective carriers of disease in a country of primitive sanitation.
So also at Debra Birhan Jock Reid found a school of two hundred pupils, of whom fifty or sixty were orphans boarded on the premises. They slept two in a bed, with one threadbare blanket ; clothes were in tatters and food appalling. Daily rations consisted of little more than dry scones and injera (the native flapjack bread made of teff) and water. Eventually, after two years of pleading and pressure, the diet was raised to a satisfactory level, largely with the help of Emanuel Abrahams, who had meanwhile become Director General of Education in Addis Ababa.
At Hadama Bartie Knight spent an hour and a half each day teaching in the school, while the dressers carried on the clinic.
Prisons were more difficult. Unless the local powers were co-operative and allowed access, little could be done. At Ambo, after a time, access to the prison was barred completely, but at Fiché a great deal was achieved to raise the standard. In Debra Birhan there were two prisons, one for minor offenders, such as wife-beaters, the other for those guilty of more serious crimes such as cattle-stealing and robbery with violence. The former was a tin affair in which prisoners of both sexes were herded together, shackled together in pairs by means of rough fetters round their ankles. The Governor was persuaded to close this prison completely and to transfer the prisoners to the one main prison in which there was ample room. The poorer prisoners were extremely badly fed, often for days on end receiving no more than a handful of dried peas; the wealthier prisoners had food brought to them by their relatives, and were even allowed to have their servants to wait upon them. Further representations resulted in improved food and bathing parades twice a week in a nearby stream, in repairs to the fabrics done by the prisoners themselves, and a separate cell for women prisoners.
Two or three times a week, sick prisoners chained together were brought to the hospital under guard, and serious cases were admitted to hospital. On one occasion a patient under guard made his getaway at dead of night, stark naked, with a temperature of 105°. Thereupon his guard was incarcerated in his place. The dresser on night duty protested his innocence of collusion by demonstrating how he had saved the hospital blankets as the prisoner made his escape by the lavatory window.
There were further experiments---a new water supply for Debra Birhan to replace the foul water holes which had previously been used; water for the hospital at Hadama to save the dressers having to go to the railway station, when the local pump broke down, to catch the drippings from the hydrant that supplied water to the engines regular sick parades for the local detachments of the Imperial Guard, the Regular Army and the Territorials, the last-named, in contrast with the other two, being a rag-tag-and-bobtail muster which drained the Treasury in an attempt to solve the unemployment problem; the treatment of goitre with iodized mixtures which quickly produced amazing results in the children; sick visiting in tukuls, especially necessary in places like Ambo and Bishoftu in which there was no room for in-patients. Entering a tukul from the bright sunlight the visitor could at first see nothing; there was no window and the air was filled with smoke from the wood fire smouldering on the earthen floor. There, huddled in a corner, the patient would be lying in a high fever surrounded by other members of the family and by its livestock large and small.
Shoa in fact demonstrated in microcosm the vast health problem of Ethiopia.
IN THE FAR SOUTH lie the Ethiopian lakes, in a broad sun-baked valley some four hundred miles long and bordered by tree-clad mountains. Here live the Sidamo to the east, the Wollamo to the west, the Borana farthest south of all. As the three provinces had hardly any medical service, it was natural that the Unit should turn its attention to them.
On 26th October 1942, as already mentioned, Hugh Brown, with an Italian doctor and an Italian laboratory technician, left Addis Ababa for Ergellum in Sidamo, the capital of the three provinces. He found that what had been a small Italian hospital building was being used partly as a stable, partly as a butcher's shop. Doors were broken, windows missing, and the roof was leaking badly. The forest had grown to within a few yards of the hospital doors, fowls lodged under the eaves and hyenas strayed into the porch at night.
After a time the hospital was cleaned up and work began. It was the familiar pattern. Work started in the out-patients clinic early in the morning, with the help of dressers, one of whom spoke four languages and acted as interpreter until the arrival of another who spoke eight. But even he was sometimes beaten, as when two Sidamos came in from the distant mountains to the east injured by a bomb explosion.
Patients came from great distances, travelling by mule from the east over the mountain passes of Mount Guramba, infested by shifta and leopards, from the Arussi country to the north and the beautiful Dilla coffee district to the south. One woman had heard in her Arussi village that there was now a Hakim at Ergellum and had mounted her mule and journeyed five days to get there.
There was accommodation for ten in-patients, and there were the usual visits to prison and school. Much of the work in the earlier months was aimed at improving the inside of the hospital and the land surrounding it. One day an Ethiopian surveyor arrived; he measured the land by foot and the angles by eye, and allotted a wide strip of woodland to the hospital running down to the river in the valley beneath. Some acres were cleared and sown, part being cultivated as a hospital vegetable garden.
To the west of Ergellum, among the Wollamo, lies Soddu. Here Ted Dunn arrived with drugs and equipment and fifty Maria Teresa dollars (£7 10s.) in his pocket to start a medical service. Four miles out of Soddu a hospital had been founded by the Sudan Interior Mission and enlarged by the Italians until it was capable of holding seventy-five patients. It was now closed and there was no money to re-open it ; fifty Maria Teresa dollars would not go far. So a smaller Italian building in the town itself was taken over, cleaned and repaired and whitewashed, furniture being provided by a very co-operative Governor. Rapidly the work developed in the trinity of hospital and school and prison. The Wollamo were a more advanced people than their neighbours, the Sidamo; they were hard-working and quick to learn, and there was prospect of training a very competent local staff. When Ted Dunn was joined by Paul Wakelin, they were able to run regular classes, and out-patients sometimes rose to 200 or 300 a day on market days, when the inhabitants came in from surrounding villages. Between May 1943 and March 1945 over 50,000 cases were treated in the out-patients clinic and 365 were nursed in the hospital.
Supervision of Ergellum and Soddu by a Unit doctor from Addis Ababa was quite impossible. When, therefore, the new party of five Unit doctors arrived, Dr. John Salter was sent down to share his time between the two centres, a journey which took three days by mule. Then a more ambitious teaching scheme was started for volunteers from the surrounding villages, a scheme which was specially welcomed by the Protestant converts made in pre-Italian times by the Sudan Interior Mission.
At the village of Wondo near Ergellum there was a sudden outbreak of meningitis. Paul Wakelin was sent there, and fortunately had available some of the F.AU. stocks of sulphapyridine. Living in a native tukul himself, he walked great distances from one tukul to another, until the epidemic was got under control. Meanwhile in his own tukul he had started an out-patients clinic, but conditions of life and work were such that the Unit after a time insisted on his withdrawal. A further clinic, with a dresser in charge, was opened at Bodditi, while John Salter was loaned for a time to work in Neghelli among the Borana on the borders of Kenya.
Well to the south-west of Addis Ababa lies the town of Jimma. It was intended by the Italians to be the main centre in that distant territory. Unfortunately, they built the town on the floor of a valley surrounded by malarious swamps. With more wisdom the hospital was built on an adjoining hill in the village of Giren.
 |
 |
 |
 |
Ted Dunn had originally come down to Jimma to assist the Military Mission doctor, who was running, with an Indian doctor, a small section of the grandiose hospital building. Ted Dunn was moved on to Soddu, where the need for him was greater, but in November 1943, when the Military Mission doctor departed, the Unit took over the whole responsibility. The short gap between his departure and the Unit's arrival had led to widespread looting, but gradually order was restored and the work built up. Dr. Alastair McLeish was sent down with Denis Roberts, now withdrawn from Wollisso; later Colin Prior, who, with Glyn Johns, had been conducting the classes for dressers at the Menelik Hospital in Addis, came down for similar work in Jimma. They were joined too for a time by George Cooper who made it his job to go round Unit hospitals to set their pharmacies in order. They found a shortage of beds, sheets, blankets, pillows, and, most disconcerting, of drugs. But gradually the work was built up, until there was room for fifty-five patients in the hospital. Sick parades daily for the Army and the police and the Territorials a smaller clinic down in Jimma itself; a sickroom in the prison medical examinations of the school, of which the Unit supplied the headmaster---it was the familiar round of activities.
It was in Jimma that Fred Wilson started a Tropical Ulcer Clinic. In the heat of Jimma tropical ulcers were specially prevalent ; beggars lay in the market-place to collect a pittance by displaying the gaping and sloughing mess on their calves or ankles. There were so many of them that there was no room for all in the hospital. So, in August 1943, premises which had been an Italian convalescent hospital were taken over, a mile or two outside the town. The buildings were poor but provided room for a main dormitory capable of holding fifty beds, a mess-room, kitchen, dressing-room, and operating theatre with showers and water-closets.
The treatment was two-fold; it involved local treatment, usually with closed dressings of plaster-of-paris after antiseptic applications, and the treatment of the vitamin deficiency which held up recovery. In many cases there were complicating factors such as syphilis or hookworm which required additional treatment.
The patients were housed and treated and taught occupations to keep them busy during the day. They made baskets and brooms and raffia mats on which to lie at night ; all the bandages used in the hospital were made on two hand-looms assembled in the grounds. From the schoolroom floated the constant sing-song of middle-aged men learning by rote the alphabet, their instructor being a senior boy from the local school. In a year 256 patients were taken in, and 213 discharged. Many of those cured had jobs found for them with a Rubber Development Unit of the British Government, operating in the forests of the south-west.
Out to the west beyond Ambo lies Lekhempti, where the hospital had been started by the Swedish Mission. It was found to be in the usual state---no beds or bedding, practically no drugs, and no surgical instruments. With drugs and instruments supplied by the Unit, Dr. Tony Husband and Gordon Hoar started a clinic, but at first patients wanting admission to the hospital had to provide their own beds and bedding. Gradually a thirty-five bed hospital was established, with an operating theatre. Daily classes were given to the dressers, some of whom made excellent progress. In fact, when Tony Husband later moved to the Hammanuel Hospital, he took with him two of them to be his theatre staff. In the course of 1944, Dr. Soderstrom of the Swedish Mission returned to Ethiopia after some years of absence, and the hospital was handed over in good running order to him. It was one of the few cases in which the Unit, when it came to leave Ethiopia, felt confident that the work it had begun would be carried on. It was a bitter blow to learn a few months later that Dr. Soderstrom had died of typhus.
As far to the east of Addis as is Lekhempti to the west, lies Diredaua. The town is in two sections, separated by a river, of which the European section on one side was a British reserved military area. It was the Mogalla Hospital in the native quarter and public health which became the Unit's concern. Donald Iles was secretary-quartermaster to the hospital, which was run with the assistance of two Italian prisoner-of-war doctors. Out-patients saw fifty to seventy-five fresh cases daily, and the 120 beds often became too few, as when there was a serious smallpox epidemic in the town and the surrounding countryside.
Finally, there was the group of hospitals and clinics in the far north of the country, more accessible from Eritrea than from Addis Ababa itself. The two main hospitals were at Adua and Gondar---Adua the scene of the Italian rout in 1896, and Gondar the remote mountain city north of Lake Tana, which was once the capital of the country and the last place from which the Italians were rooted out in 1942, several months after Addis Ababa had fallen.
The first Unit party to go north to Adua and Gondar had dropped Douglas Lister at Dessié to act as quartermaster-secretary to the hospital, a wooden structure under a Military Mission doctor. The work, in which Douglas was followed by Glyn George, consisted of the usual tasks allotted to the secretary, the preparation of disease returns, responsibility for accounts, the payment of staff, the purchase of foodstuffs.
It was on Christmas Eve 1942 that a party of three arrived in Gondar---Jim Wilson to be secretary of the hospital, Albert Tomlinson to be in charge of the pathological laboratory and stores, and Eric Ankers to act as ward master. The hospital was one of the largest in Ethiopia, and its expansion was limited only by money and the time which the Military Mission doctor could give to it, for he had two battalions of the Ethiopian Army to look after instead of the normal one. The very remoteness of the hospital caused additional difficulties. Before a message could get through to Addis Ababa, the time for action was normally well past. The development of the hospital followed the regular pattern; the issue of food was regularized, proper registers were kept, a small laboratory set up with F.A.U. equipment; the Army battalions on the shores of Lake Tana were vaccinated and sick parades were held for the Territorial Army, with a special V.D. clinic. Prison, school and water system received attention and regular classes were held for dressers. It took five months to arrange and catalogue the vast medical store, but in time the hospital came to have as high a standard as any in the country.
Further north in Adua, Ian Robinson joined a Military Mission doctor in what was the only hospital of any size in Tigrae, an area twice the size of Wales. When the doctor was in due course moved, John Wyon, a Unit doctor, was sent up. He and Ian had the hospital redecorated and a new operating theatre built. Between January 1944 and March 1945, 1,050 patients were admitted, fifty-five beds being occupied on an average, and 574 operations requiring an anæsthetic were performed. They too had classes for the dressers and public health schemes in the town, with visits to the school and prison, where a year's protests seemed to have produced at least a veneer of cleanliness, while an excellent Ethiopian midwife trained in Asmara meant that the hospital had an unusually high number of obstetrical cases.
Based on the hospital there were clinics in the town of Adua itself and in the holy cathedral city of Axum, which between them dealt with 15,000 patients. There were also two smaller dispensaries. John Wyon visited every six weeks further clinics in Makalle and Adigrat. Ernest Grimwood and Brian Phelps were in Makalle in the autumn of 1943 when the Tigrae rose in revolt against the central government and the town fell into the hands of the rebel chief, Belatu Haile Mariam. The fighting meant a rush of patients for Adua Hospital; for the two in Makalle it meant more excitement than was healthy for them, and after being held for a time they were glad to get out after Ernest had visited the rebel chief in his mountain lair to secure a safe conduct. A new clinic was started under John Grimwade at Adigrat, where, as elsewhere, in addition to an out-patients clinic, school teaching and public health were undertaken.
By the summer of 1944 the Unit had a network of hospitals and clinics giving treatment every week to many thousands of people who would otherwise have died or lived on in wretchedness.
IN PRACTICALLY EVERY TOWN and village in which they worked, Unit members, as already shown, did what they could to promote interest in public health and to ensure that elementary precautions were taken. In Jimma Fred Wilson had an extensive programme of malaria control which at least prevented the disease from reaching hyper-epidemic proportions in a town for which the only permanent solution seemed to be wholesale removal from its swamps to a healthier site. In Hadama too malaria control in the Awash valley was organized.
But it was in Diredaua and Addis Ababa that the Unit undertook public health work on a larger and more ambitious scale. Jack Harris and Gilbert Root in Addis, Geoffrey Hunt and Ted Fitch in Diredaua supervised the sanitary services. In Addis Ababa sanitary inspectors were given training; the cleansing arrangements were made more thorough ; public spaces cleaned up ; over 100,000 people were vaccinated ; latrines were built, regulations drawn up concerning wells, shops, slaughter-houses, tej shops and catering establishments. But then came the inevitable chicachic---an expressive Amharic word for a bothersome spot of argument. The control of public health services had been a bone of contention between the Medical Directorate and the municipalities long before the Unit arrived on the scene. On this occasion the Directorate lost ; the control of the services reverted to the municipal authorities, the Unit men were transferred to other work, and most of the good achieved was again undone.
In Diredaua there was better progress. There, after an extensive vaccination campaign organized by the Unit to combat an outbreak of smallpox in the town and in the surrounding country, work was similarly started on the sanitary services. There was a scheme of malaria control in the river Laga Arre ; sanitary police were employed ; prisoners cleaned up the filthier parts of the town; regulations were drawn up to check he disposal of refuse in the streets and the normal custom of urinating and defecating in public ; a poorhouse was started to accommodate and feed the sick paupers who were lying, and often dying, at the roadside ; the water supply and slaughter-houses were regularly examined. As Donald Iles was secretary of the Magalla Hospital, close co-operation between him and the public health services was possible. In due course a Sudanese who had been a sanitary inspector in Khartoum was sent down by the Medical Directorate and he was able to take over the work finally in March 1945.
In education too most Unit members had some hand, if only through spare time teaching in the village school. The state of some of the schools has already been described. It was obvious that the key to any permanent development was education. There was ground for hope when Emanuel Abrahams became Director of the Ministry of Education, and in 1944 there were four members of the Unit regularly attached to him-Douglas Lister for work in the office, Selby Clewer as architect of the Department responsible for improvements and developments in the schools, and Bernard Fisher and Victor Menage as headmasters, Bernard of the Asfa Wassen School in Addis Ababa, Victor of the school in Jimma.
The Asfa Wassen Model School in Addis Ababa, housed in a stone building with several wooden annexes, was a boarding school for over two hundred orphans, mainly pauper children picked off the streets. The great handicap, as always, was lack of money. The boys often missed meals altogether, and were constantly underfed. But the school became well ordered, with instruction in Amharic, English, arithmetic, hygiene and other subjects, regular medical inspections and P.T. There was in the midst of hopeless poverty an air of keenness and interest which would do credit to many an English school. For months the staff were buoyed up by the hope of transferring the whole school to better buildings, which were ready to receive them, but money was the constant stumbling block.
Victor Menage found himself taking up residence in Jimma with the imposing title of "Director of Education for the Province of Jimma and its Dependencies," but he found in practice that this meant being headmaster of the local school.
"In the main building there were theoretically 450 boys, though no process of addition on my part could bring the total above 200 actually attending. The subjects taught were Amharic, drill, Arabic, English and a little arithmetic, in that order of importance. Most of the boys are Amharas and, besides Gallas, there are Arabs: Indians (a sprinkling), and the despised Shanko, negroes from the forests. There are only a very few boys who do not speak Amharic, and they are in the bottom class battling with the alphabet.
"The main difficulty is that, when a child can read and write a bit, his education is triumphantly concluded. I should be very abashed to think that I was merely helping to swell the number of wiriquet writers in Government offices."
It was mainly for educational work that those members of the Unit who stayed on after the official withdrawal, remained. In the face of seemingly insuperable problems, they were convinced after three years in the country that it was the one and only answer.
TOWARDS THE END OF 1944 the Unit was fighting a losing battle against increasing difficulties. Problems inherent in the struggle of a backward country to find its feet they were, of course, very ready to accept ; it was in fact the job which they had gone to do. But there were further difficulties, some undoubtedly avoidable, others arising inevitably out of the Unit's own position as a temporary organization trying to avoid becoming too deeply committed in what ought to be permanent work.
Colonel Maclean had resigned from the Medical Directorate, and he was succeeded by a lay Ethiopian. The financial position of the Directorate and the control of its budget were becoming no easier. There was also constant trouble over the supply of drugs, trouble by which any attempt to develop medical work was hamstrung. In any country valuable and dangerous drugs have to be rigidly controlled. It was particularly important in a land where a great deal of valuable material had already got into private hands, and some drugs, especially those for treating venereal disease, could almost be regarded as currency. The Italian doctor who was in charge of the Central Medical Store had been arrested and a lay Ethiopian had taken his place. He was in turn put on trial for stealing drugs and yet another Ethiopian appointed. At last the Middle East Supply Centre put its foot down and refused to let any new drugs enter the country to make up what deficiencies there were unless the Central Store was under adequate technical control. The story of the subsequent negotiations and bickerings need not concern us. It all contributed to the growing handicaps to any satisfactory work.
More intangible was the difficulty which the Unit, in company with other European workers, found in achieving the trust and co-operation of certain Ethiopians. The common people they found friendly and humorous and helpful once the initial suspicion of the faranji had been broken down; but in other quarters there was a growing impression of resentment or lack of interest. On the one hand was the country's crying need of assistance ; on the other a suspiciousness of any interference from outside.
There is no doubt that the Unit for its part had something of the impetuosity of youth. It was very easy to become petulant, and to fall into the trap of applying European standards to a situation to which such standards were obviously alien. The strain too of working in a backward country, especially in lonely outposts in the provinces, was considerable, and a temporary organization anxious to see signs of progress did not take kindly to the attitude summed up in those untranslatable words, which were on every tongue in Ethiopia, ishi naga. The maleesh of the Egyptian is its nearest equivalent---"Never mind" or "Don't worry me now, it will do just as well tomorrow." The country needed people with the zeal and patience of the best type of missionary, prepared for a life-time, not a year or two, and very few of the Europeans in the country came up to that standard.
Such difficulties undoubtedly contributed to the Unit's decision to withdraw. But the main reason for pulling out was that given all along---the Unit was a wartime body and there were signs that the end of the war was not far off. Most members would gladly have stayed on for a further period if by so doing they could prevent the work which they had begun from collapsing. But it would be a mistake to carry on if that meant the postponement of more permanent arrangements. In November 1944 the Unit believed that there were methods available to the Ethiopian Government for replacing it, and that only by the announcement of a clear decision to withdraw could it bring home to the authorities its own temporary nature. So notice was given that withdrawal would take place between February and May 1945. When the time came for the main body to depart, some members remained under other auspices. Michael Vaízey, who had been joined by his wife and family, became Director of the Menelik Hospital ; Selby Clewer, the architect, and his wife continued with the Ministry of Education; Norman Boyes, Ken Tipper and Victor Menage carried on educational or welfare work under the Ethiopian Government or the British Council.
The provincial clinics were handed over to native dressers, some keen and able to inspire confidence that the work would continue, others without much substance of training or knowledge to support them. The Unit's most ambitious effort, the complete control of the Hammanuel Hospital, came to an end because the hospital was closed, and its patients moved to the Menelik. The Leprosy Camp was taken over by a capable Australian nursing sister. At Gondar Jugoslav and Indian doctors were installed, and at Jimma two Italian doctors.
It was with great regret that the Unit members returned in small groups to England in the spring and early summer of 1945.
Their three years had been very far from wasted. In fact, a visitor to Addis Ababa and the remote outposts in the provinces could not but be impressed by the fact that man for man Unit members in Ethiopia were carrying more responsibility than in any other country. A great deal was achieved, but it was a disappointing end. There would be memories of indifference and obstruction and lack of understanding in high places, a feeling that the foundations which they had hoped to lay had not been laid. But there would be memories too of hard work, of pain relieved and lives saved, of the beauty and mystery and fascination of the country, the friendliness of ordinary people and their lively sense of fun, the small boys with their coxcombs and twinkling eyes, the small girls with their bald patches surrounded by a mass of frizzy hair, the appreciation shown by so many of what the faranji had tried to do for them.