
Mr. President, colleagues, ladies and gentlemen: I am to discuss today the question of transportation of the wounded, which is one of the problems of modern warfare---perhaps the greatest. Compared to the progress which has been made in perfecting the means of destruction there is no question that the methods of evacuating the wounded are certainly very crude and open to great improvement.
The advent of the automobile should have been the means of simplifying and ameliorating these methods and of making military sanitation equal to emergencies of modern war.
As we shall see, this has not been the case, because the railway is still the main medium of transport, and motor ambulances are not utilized to the extent that they should be.
One of the main reasons why the evacuation of the wounded is often so badly carried out is that the lines utilized for this transportation are often the same as those that are used for the conveyance of troops, food and ammunition. This has given rise to that implacable formula so often quoted, Ammunition first, food second, wounded third. This, to my mind, is a cruel, senseless and useless maxim. How many human lives have been sacrificed to it!
The task of evacuating the wounded at its best is undoubtedly a complicated one for many reasons: There is no work which undergoes such unexpected and startling variations. On certain days, the number of wounded to be evacuated (as was the case some weeks ago) did not exceed 300 all along the French front, while again there may be 10,000 or 20,000, or even more, in a day, as in the battle of the Marne. 'What still further hampers the Service de Santé is that the greater the number of wounded at a given point the more difficult the evacuation becomes, because of the congestion of the various lines of transportation.
When one fully appreciates the tremendous difficulties which confront the military surgeon in his work at the front, one can but admire his courage, his devotion and his resource. Our experience in the transportation of the wounded teaches us that there is a vast difference between theory and practice. When one opens a book on the subject "Troussaint's Service de Santé en campagne" or any other treatise on the subject, one finds a great many precise rules and regulations dealing with the transportation and evacuation of the wounded. The handling of the wounded becomes apparently a question of military tactics. It would seem to be a very simple matter, but how different are the actual facts! There is no other service which is subject to so many daily and hourly variations and in which the conditions are so constantly changing.
We all know that there are three different phases in the movements of an army or of a battalion: It may advance. remain stationary, or retreat. The various military operations are. of course, capable of all sorts of variations, any one of which may in a moment create for the Sanitary Service situations of the greatest difficulty.
If the army advances, the situation is very simple, because the wounded become each minute further removed from the enemy, and it is comparatively easy to handle them. When the army remains stationary, as in the present form of trench warfare, the situation is also very simple, because the Sanitary Service has ample time to organize its work.
But when the army is in retreat the difficulties begin. The enemy advances with more or less rapidity, and the Postes de Secours and the field hospitals must be evacuated without delay. Frequently the patients can be removed to the rear, but too often the evacuation cannot be effected rapidly enough, and the wounded must be left where they are in charge of one of the surgeons who remains behind. Many of them fall into the hands of the enemy.
These three phases have already been exemplified in this war:
1. The retreat from the north after the battle of Charleroi.
2. The advance during the battle of the Marne.
3. The stationary situation created by the present trench warfare which has lasted for so many months.
The allies were unfortunate in having the most complicated situation to cope with at a time when the sanitary organizations were least able to meet it. I cannot report personally how the wounded were transported at that time. There is no doubt that a large number fell into the hands of the Germans.
Our actual experience began with the German retreat in the battle of the Marne---the advance of the Allies. At that time the problem which confronted the Sanitary Service was twofold: The hospitals of the North had to be evacuated, and in addition, some 112,000 men who fell during this memorable battle had to be transported to the various hospitals. This, too, came at a time when the Service de Santé was still badly prepared for its work. Ours were the only ambulances which were ready at that time. Our souls were harrowed by tales and sights never to be forgotten---hundreds abandoned without food and drink for days in half ruined churches or schools, or again lying on straw in shunted cars which could not be sent forward on account of the railway being used by ammunition and troop trains. The mere mention of the battle of the Marne evokes souvenirs of the many expeditions we made to Meaux, Lizy-sur-Ourcq, Crépy-en-Valois, etc., and it is hard to refrain from recalling here some of our experiences.
It was during this period that we gained much of our experience in transporting the wounded from the advanced lines. We were kept very busy, our motor ambulances being the only ones which were in readiness to respond day and night to the calls of the sanitary authorities.
Before describing the various means of transportation I wish to say a few words about the obligations which we owe to the wounded. When we see the wounded arriving at our door we are too apt to look upon them as subjects to whom we intend to give the best of care, but for whom we do not have the keen, deep human sympathy which we should feel, did we but realize the physical and mental suffering through which they have just passed. It is well for us to remember the agonizing hours spent on the battlefield, and the complicated and nerve-racking journey which has finally landed them at our doors.
Dr. du Bouchet spoke very feelingly at our last meeting of our duty to the men who have fought bravely for their country. Our duty should begin not only with the treatment given them to alleviate their physical suffering, but the very minute we meet them. These men have left their homes, their occupations, their wives and their children to lay down their lives if need be for their country. They have fulfilled their duty to society, and our obligation to them, the humblest of them, is to treat them with the greatest gentleness and patience.
In order to evoke in your minds a complete picture of that journey (which so often, alas! ends in a tragedy) which the wounded soldier takes from the firing line to our hospital, let us start on the battlefield itself. For a description of what generally happens on the firing line I am indebted to our military colleague, Dr. Perrin, who was wounded near Arras, in the accomplishment of his duty, and who, fortunately, has almost regained his health in the American Ambulance.
I think there is great interest in following the wounded soldier from the battlefield until he reaches the point where our base hospital comes in contact with him. If he is wounded in the open, he falls on the firing line, and tries to drag himself to some place of safety. Sometimes the fire of the enemy is so severe that he cannot move a step. Sometimes, he seeks refuge behind a haystack or in some hollow or behind some knoll. Generally a number of wounded will collect in the same place. This is called by the picturesque name of nid de blessés or "nest of wounded." If the artillery or rifle fire is particularly severe, they will remain here till darkness comes on. In the meantime they apply a dressing to their wounds or have them dressed by some comrade. Under the cover of darkness, those who can do so, walk with or without help, to the Poste de Secours or First Dressing Station which, in open warfare, is situated from 500 to 1000 metres from the firing line, generally in some protected spot. As we shall see later on, in trench fighting the nid de blessés becomes the Poste de Pansement in a third line trench.
Of course there are various ways in which the wounded can get to the Poste de Secours.
Stretcherbearers are sent out to collect the severely wounded. Sometimes mules are used, with an arrangement of sideseats called a cacolet, or a two-wheeled push cart, similar to the Japanese pousse-pousse. This vehicle is of the greatest service when the roads are good, and Dr. Perrin recounts that he succeeded one night in transporting 18 badly wounded soldiers from a spot 50 metres from the German lines to a point several kilometres back, in a very short space of time.
The wounded are not kept very long at the Poste de Secours. Their wounds are dressed, and in the case of fractures, improvised splints are applied, and the patients are evacuated as speedily as possible. This is accomplished by a system of ambulances, which operate from another service called the Service de l'arrière, but the number of motor ambulances is wholly inadequate, and this is a serious flaw. I am told that frequently the ambulances do not make connections, and that the surgeon of the battalion in charge of the Poste de Secours must get his wounded out as best he can, requisitioning for this purpose the peasants' carts and wagons. The dressing station does not part with its stretchers, so the wounded are placed on straw spread on the bottom of these carts without springs, and thus they are conveyed during five or six hours before they reach the sanitary train or temporary field hospital. What torture many of them must endure, especially those with multiple fractures!
This description applies to open warfare such as existed in the early stages of this war. The sanitary service, as well as the combatants, has been obliged to adapt itself to these new and strange conditions, and I am quoting from Ferraton, who describes the practical workings of the service under his direction.
The hardships of the soldier in this trench fighting have been shared by the military surgeon and his associates, and one must express the highest admiration for their coolness and courage under most trying conditions. Here, there is no Geneva convention. The medical corps is exposed to the enemy's fire in exactly the same degree as the soldiers. The military surgeon, as well as the stretcherbearer, remains behind the combatants, in third line trenches, in trenchrooms, covered with transverse logs and sod. As soon as a soldier is wounded, the stretcherbearers go to get him by means of the communicating couloir or trench. The ordinary stretcher is too long to be used in the tortuous and abrupt angles of these trenches. It has been found more convenient to use a sort of a palanquin made by suspending a canvas sling from a wooden pole. An ordinary chair is often the most convenient means for transporting the wounded from the first trench to the so-called Poste de Pansement (dressing station). This Poste de Pansement is often situated in a second line trench.
In this subterranean room, dimly lighted, the dressings are applied, splints adjusted, hemorrhages arrested by means of an Esmarch bandage, and warm drinks given. There is generally at least one of these Postes de Pansement to each battalion. As soon as the shelling permits, the wounded must be carried to the Poste de Secours, which is generally situated a hundred yards or so in the rear, in some house. The wounded are carried to the heads of the communicating trenches, and at a favorable moment, transported on litters, either with or without wheels. At the Poste de Secours some immediately urgent operations may be performed, such as ligating for hemorrhage, tracheotomy for threatened asphyxia, etc. At this point ends the regimental service, and the divisionary surgeon takes charge. He has disposal of various horse-drawn ambulances or two-wheeled push carts.
In one particular division described by Ferraton (Société de Chirurgie of 16 March) the Poste de Secours was in a subterranean chamber hidden under a hay stack, and another was situated in the cellar of an abandoned house; in each case relatively safe from the shells which were bursting all around.
From the Poste de Secours the wounded are carried to the so-called Ambulances, of which there are two kinds:
1. The first line divisional ambulances.
2. The ambulances of the second line (Ambulance de Corps d'Armée ou de deuxième ligne).
The first line ambulances, which, during the prolonged trench warfare have remained stationary, are generally, under ordinary circumstances, very mobile. The whole service can be packed on a few horsedrawn carts. They possess no beds, and are generally established in abandoned houses, the wounded being placed on clean straw. The duty of these ambulances is to receive the wounded sent by the regiments, perform the most urgent operations, but, more particularly, to make a choice of the wounded for distribution, hence the name Ambulance de Tri.
1. The slightly wounded are kept near the front.
2. The moderately wounded, who can stand a long journey, are sent to a sanitary train.
3. The very seriously wounded, who can only be transported a short distance, are sent to some neighboring ambulance.
The first group will be transported to a dépôt d'éclopés, the second to the evacuation hospital of the army corps, and the very severely wounded to a neighboring fixed surgical ambulance.
This latter is what is called a second line ambulance. It is situated in some neighboring village where there are comfortable buildings, and where a good surgeon can perform many urgent operations on abdominal and head cases.
These hospitals may have a capacity of 50 to 100 beds and would quickly become overcrowded if the patients were not being constantly evacuated, either by means of a sanitary train to a base hospital, or, if too weak, to some surgical hospital of a neighboring village. The wounded have, therefore, successively passed by the Dressing Station (Poste de Pansement), the Poste de Secours, and the Distributing Ambulance (Ambulance de Tri). In this latter place they may remain not over 15 hours, often only a few hours, and from here, according to the gravity of their wounds, they are transported by horse-drawn vehicles or motor-ambulances to the dépôt d'éclopés, the evacuation hospital, or the ambulance hospital. If the service is well done, the wounded are delivered at the ambulance hospital from four to eight hours after having been picked up, and, in many cases, within two to three hours.
At the immobilized ambulance hospitals, the badly wounded cases are supposed to be kept, i.e. the head, chest and abdominal cases. The others are forwarded to the sanitary trains or canal boats or sanitary ships to be distributed according to the gravity of their lesions to more or less distant hospitals. The head station of these sanitary trains is called the Gare d'Origine d'Etapes, and the station of arrival is called the Gare de Répartition. There are two such depots in Paris, the Gare d'Aubervilliers and the Gare de la Chapelle St. Denis, with which our ambulance drivers are very familiar. This latter station, where sometimes 2000 wounded arrive in a day, is in charge of Dr. Quénu and is admirably organized.
This is where I shall try to prove that the methods of transportation could be greatly simplified by a better use of motor ambulances. You see how complicated the machinery is for transporting the wounded from the firing line, and how important it is that every stage of that complex journey should be carefully planned and carried out. By the judicious use of motor ambulances much of the changing from one vehicle to another would be obviated.
I must here give a short description of various forms of motor ambulances, and I must be forgiven if I speak a little more in detail of our Ford ambulances which have stood the test of nearly six months' steady use, both in field and base work.
In the early part of the war, whilst the committee was organizing this section of our American Hospital, I remember one day, on coming from a committee meeting, at the offices of the American Radiator Company, in Bd. Haussmann, seeing one of these cars standing in front of the door, the chassis being furnished with crude ambulance bodies made from wood of packing eases. It was a surprise to us. We knew they were being built, but we did not expect they would be ready so soon. I remember my emotion when Dr. du Bouchet and another member of the committee rode round the block, whilst we anxiously awaited their return and their opinion. The car was pronounced most comfortable, and it has since justified that verdict.

That was the first appearance of the Ford ambulance, and while some modifications have been made as to the details, the principle remains the same. The advantage of this car for work at the front is at once apparent. Its lightness, its exceptional clearance from the ground, and the power of its engine make the car a perfect one for work immediately behind the firing line. In the North, when the roads were muddy and bad, it was the only car which could get off the road into the mud to allow a convoy to pass and yet get back upon the road without the aid of a tow-rope. In the East, in the Vosges mountains where one of our sections is working in Alsace, they take the hills so well that the French soldiers have nicknamed them "the goats."

Though we have not modified the general shape of the ambulance, we have gradually improved the model, with regard to the comfort of the patient and also of the drivers. We found that a third stretcher would be of help, and this has been supplied. This emergency stretcher is placed on a wooden frame, which can be either strapped out of the way against the roof of the car, or secured in the center of the car above the other two stretchers.
Three lying-down cases are all that a Ford car can safely carry over rough roads without straining the springs. As for sitting cases, four can be accommodated in each car. At first we allowed the wounded to sit on the floor with their backs against the sides of the car. Then we thought seats would be better, and we now have two transverse seats for four sitters.
So far as the Ford is concerned, I feel that it has a great future as an ambulance. In the transportation of the wounded the patients are most comfortable. At present, the wounded are being transported over 60 kilometers over rough roads to our branch hospital, at Juilly, and the men all declare that they much prefer to ride those forty miles to the journey of eight or ten miles which they had to make from the front to the first clearing hospital in such vehicles as I have just described---springless carts, etc. In fact, many of the men fall asleep in our ambulances during the journey to our hospital.

The larger cars of the Daimler or Wolsley types, carrying four lying to six or eight sitting, are good for base work, but they are too cumbersome to be able to run very close to the front. On the other hand, the Ford, with its low outline, can creep very close to the firing line without attracting the fire of the enemy.
To resume, motor-ambulances may be made to carry two, four or six lying cases, or from four to eight sitters. The stretchers may be pushed into the car from behind or from the sides, as in the Austrian model, and in a new ambulance invented by Com. Denain, of Versailles, which is now being made for the French Army, of which I am showing you an illustration.
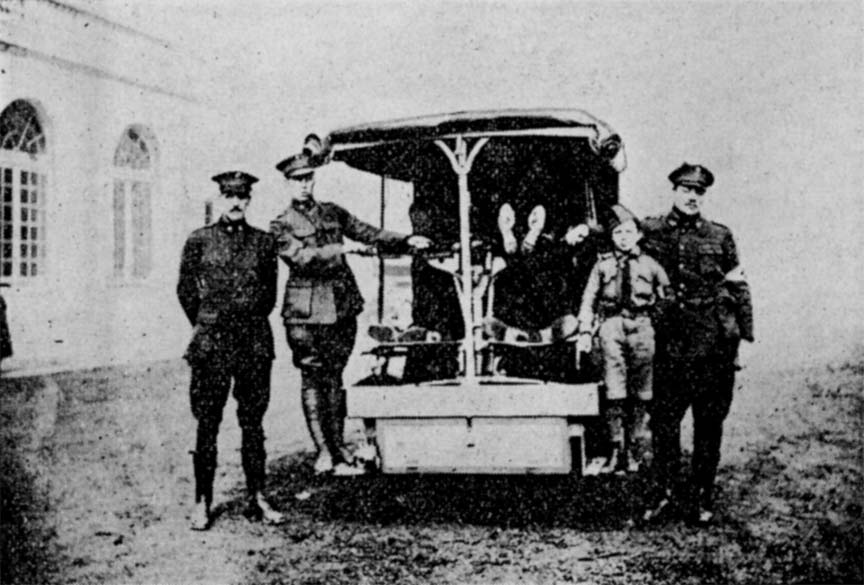
This new ambulance is very ingenious and very practical. It loads from the side. The whole frame supporting the four stretchers rests on two transverse buggy springs, which absorb the shocks and make riding over rough roads very easy, obviating longitudinal or transverse vibrations. All these points may seem trivial, but they are of the utmost importance so far as the comfort of the patient is concerned.

Many systems of suspension of stretchers based on spiral springs do not take this into account. I have several times tested this form of suspension by riding around over rough roads---and have found the vibrations most disagreeable, and realized bow agonizing such a trip would be to those suffering from fractures.
The same criticism applies to the three-stage apparatus installed in so many of the sanitary trains. I refer to the Brechot-Deprez-Ameline suspensions in which the stretchers are also supported by spiral springs.

The conclusions are obvious: the greatest comfort of the patient is obtained when the stretcher is placed directly on the floor of the ambulance (as in the Ford), on rails (as in the Daimlers), or on rigid arms (as in the Denain). If placed on springs these must not allow of a transverse or longitudinal movement, but only of a vertical one.

In the transportation of the wounded the comfort of the patient should always be the first thought. The most painful injuries are compound fractures of the femur, and transportation is almost impossible unless the limb has been immobilized in some way. In our experience, the following simple appliance which Dr. du Bouchet taught us to use, was found invaluable. It consists of a double pillow filled with excelsior, which is placed round the limb and held in place by means of wooden splints, the whole secured together by means of straps and buckles.
I was impressed with a metal extension splint which Dr. Blake demonstrated to us at our last meeting. I believe this would bring even greater comfort to the wounded than our splint pillows.
The necessity of keeping the wounded warm during transportation is of paramount importance. It must be remembered that these poor men are generally suffering from traumatic shock, and that they easily get chilled. Even though they are covered with blankets, they lie on the cold canvas of the stretcher, with no blanket under them. We, therefore, tried to find a method of heating the car, and to keep the cold air out we secured the canvas sides and back.
One of our members tried to utilize the heat of the exhaust pipes to warm the inside of the car. Though our experiment was not a success through a mechanical error, I am quite sure that the idea is a good one and could be worked out if the season were not too advanced for heating to be necessary.

In most cases sufficient heat can be obtained from a hurricane lamp which is kept lighted, suspended from the ceiling.
Now let me say a few words about sanitary trains, of which, as you know, there are three kinds: the improvised, the permanent, and the ordinary passenger train used for the sick or slightly wounded.

Unfortunately, our experience during the battle of the Marne taught us that there was a fourth train used for the transportation of the wounded, though it could hardly be called sanitary. This was composed of cattle cars which had been used for conveying horses to the front.
Of course the military operations were such that there was no time for any attempt to establish a sanitary train. Straw was spread on the floors of the cars and the wounded placed on it. It was at that time that so many of the wounded contracted tetanus and developed gas gangrene. Many lives would have been saved if a little time had been taken to clean and disinfect the floors of these cars before placing the wounded upon them.
The most common train is that composed of baggage or cattle cars with the Brechet Ameline apparatus in either end, consisting of three tiers of three stretchers each, each car carrying eighteen wounded. In winter a little stove is placed in the middle.
The best train that I have seen is composed of second or third class compartments, with lateral doors, which permit the stretchers to be easily carried in and out (but it must be recalled that portières vary in width of opening, many of them being too narrow to permit of the passage of a stretcher.

The carrying capacity of these trains is 250 to 350 wounded, about four-fifths of which are sitting cases; in other words, there are but 60 to 70 lying cases in each train. There are about 20 orderlies, and one surgeon (rarely an assistant surgeon) to each train.
Unless the cars are intercommunicating, the surgeons can inspect his cases only at the stations, and these are sometimes three to six hours apart.
This means that the wounded are practically without medical supervision during the whole duration of the trip, and when the train reaches the "Gare d'évacuation" or Distributing Station the methods of determining the gravity of the wounds are wholly inadequate. Fortunately, this service has been greatly improved.
Another defect in the system is the method of feeding the wounded. Often there is no provision for feeding them on the trains, and this is carried out at the stations where the infirmaries are established. Here the soldiers are stuffed with unsuitable eatables often, which causes indigestion and other troubles for those who are unable to take solid food.
The already lengthy journey is made almost interminable by frequent stops. The speed of the train is almost 40 kilometers an hour, and the trip from Amiens to Bordeaux, for instance, would take 48 hours. If the feeding of the patients was attended to on the train, the duration of the trip could be reduced one half. This has been tried recently on some of the trains with success, a restaurant car being attached for the feeding of the wounded and the personnel.
I want to speak of a little experience which I had (but fortunately this condition has been corrected now). I have seen a surgeon going from car to car, simply asking the orderlies if any of the men complained. If none complained (and do we ever hear these brave soldiers complain?) they were allowed to remain where they were and sent on to some more or less distant hospital in the provinces, many deaths resulting from the delay.
Another means of transportation is the canal boat or Péniche Sanitaire. I have had no experience with this method of transportation, but it seems to me that its great objection is that it is very slow and keeps the wounded from reaching a well-equipped hospital quickly.
I saw some magnificent sanitary ships at Boulogne, used to transport the British soldiers to England. This is undoubtedly one of the best means of evacuating the wounded, particularly when the sea is calm.
To resume: The conditions to be met in the transportation of the wounded are comfort, speed and safety. The first two we have dealt with, and the question of safety I will now consider. Safety implies not only the proper treatment of their wounds, but also the proper precautions against danger of contagion from the medical cases.
In the beginning of the war there were practically no medical cases, but as the war goes on, the medical cases, among which is a large proportion of contagious diseases, are increasing in number. At least one-half of every sanitary train is composed of medical cases. They try to separate the contagious cases in the train, but it is very difficult to carry out this isolation when the surgical and the medical cases are not kept entirely apart. This defect in the transportation system is a very serious one.
To distinguish the cases readily, the soldiers should be carefully tagged with cards of different colors; for instance, red for surgical, blue for medical and yellow for contagious cases.
Having described, very imperfectly, the various methods of transportation now in use, I want to say a few last words on what I consider would be the ideal method of evacuating the wounded from the front. I should like to see the trains used only for the lightly wounded and medical cases, while the severely wounded should be conveyed by motor ambulances directly from the firing line to the temporary or even to the base hospitals.
This plan should be realized by the use of motor ambulance convoys attached to each army, and assuring a regular service between the first dressing stations or first clearing hospitals, and a base hospital. This would do away with the various and painful changes, the exhausting waits and the inevitable delays. I am sure that this would mean the saving of many lives.
I have already been too long, and there is no time to describe our own ambulance organization. Suffice it to say that it is fitted for just such work. Our units of 20 ambulances with a staff car and a repair car could be multiplied ad infinitum, and would be admirably suited for this convoy work.
It is with legitimate pride which should be shared by all Americans, that I am able to report that our various ambulances driven by volunteer Americans, have carried to date over 26,000 wounded soldiers, French, British, Indian, Belgian and German. Our American ambulances are now familiar objects all along the line. It is quite a common occurrence for our men to evacuate wounded from a sanitary train in Paris who have already been carried from the first dressing stations at the front to the head station of the sanitary train fully 200 miles from Paris.